

Associations of resting heart rate and dyslipidemia with prehypertension and hypertension among HIV/AIDS patients
-
摘要:
目的 探索HIV/AIDS患者中的静息心率(resting heart rate, RHR)过快和血脂异常与正常高值血压/高血压的关联及其交互作用。 方法 采用横断面研究的方法,基于浙江省台州市2017―2019年“HIV与衰老相关疾病前瞻性队列研究”基线数据,纳入分析30岁以上的HIV/AIDS患者。采用Logistic回归分析模型分析HIV/AIDS患者患正常高值血压/高血压的影响因素,用相乘模型探索RHR过快和血脂异常的交互作用。RHR过快定义为RHR>90次/min;血脂异常定义为TC、TG、LDL-C升高或HDL-C降低。 结果 共1 645例HIV/AIDS患者纳入分析,其中正常高值血压和高血压的患病率分别为42.8%和28.1%。15.8%(260/1 645)的研究对象的RHR过快,59.2%(974/1 645)存在血脂异常。多分类Logistic回归分析模型结果显示,调整年龄、性别、BMI、腰臀比和TC之后,TG升高和RHR过快是正常高值血压(aOR=1.56, 95% CI:1.14~2.13, P=0.005;aOR=1.60, 95% CI:1.06~2.43, P=0.026)和高血压(aOR=1.94, 95% CI:1.37~2.75, P < 0.001;aOR=1.95, 95% CI:1.20~3.18, P=0.007)的独立影响因素。同时,TG升高和RHR过快对正常高值血压(P=0.017)和高血压(P=0.032)均存在负向相乘交互作用。TC、LDL-C及HDL-C异常与RHR过快对正常高值血压和高血压均未观察到交互作用。 结论 RHR过快和TG升高是HIV/AIDS患者正常高值血压和高血压的独立危险因素。此外,RHR过快和TG升高之间存在负向的相乘交互作用,提示RHR过快可能降低TG引起致高血压发生的阈值,其机制需要进一步研究去阐明。 Abstract:Objective To assess the associations of elevated resting heart rate (RHR) and dyslipidemia and their interactions with prehypertension and hypertension among HIV/AIDS patients. Methods A cross-sectional assessment was conducted among 1 645 HIV/AIDS patients over 30 years old from the baseline survey of Comparative HIV and Aging Research in Taizhou (CHART) between 2017 to 2019. Multinomial Logistic regression model was used to assess the factors associated with prehypertension and hypertension. Multiplicative model was used to explore the interaction between elevated RHR and dyslipidemia. Elevated RHR was defined as > 90 beats/min; dyslipidemia was defined as elevated total cholesterol (TC), triglycerides (TG), low-density lipoprotein cholesterol (LDL-C) or decreased high-density lipoprotein cholesterol (HDL-C) levels. Results Among 1 645 HIV/AIDS patients, prevalence of prehypertension and hypertension were 42.8% and 28.1%, respectively. 15.8% (260/1 645) of the subjects had elevated RHR, and 59.2% (974/1 645) had dyslipidemia. After adjusting for age, sex, body mass index, waist to hip ratio and TC, elevated TG and elevated RHR were independently associated with prehypertension (aOR=1.56, 95% CI: 1.14-2.13, P=0.005; aOR=1.60, 95% CI: 1.06-2.43, P=0.026) and hypertension (aOR=1.94, 95% CI: 1.37-2.75, P < 0.001; aOR=1.95, 95% CI: 1.20-3.18, P=0.007), and there was a negative multiplicative interaction between elevated TG and elevated RHR with prehypertension (P=0.017) and hypertension (P=0.032). No interaction was observed between abnormal TC, LDL-C, HDL-C and elevated RHR on prehypertension and hypertension. Conclusion Elevated RHR and elevated TC are independently associated with prehypertension and hypertension in HIV/AIDS patients. The negative interactions between elevated RHR and elevated TC on prehypertension and hypertension suggest that faster RHR is likely to reduce the threshold for TG levels to cause hypertension. Further studies are needed to reveal the underlying mechanism between RHR, TG and hypertension. -
Key words:
- Acquired immunodeficiency syndrome /
- Resting heart rate /
- Dyslipidemia /
- Hypertension /
- Interaction
-

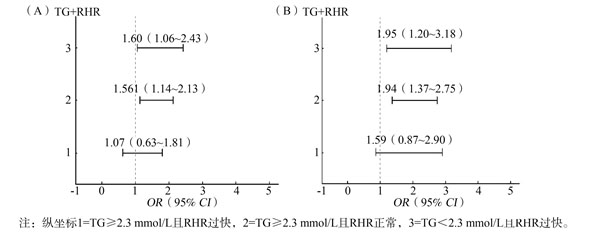
图 1 TG和RHR对正常高值血压(A)和高血压(B)的交互作用分析
Figure 1. Interactions of TG and RHR on prehypertension(A) and hypertension (B)
表 1 不同静息心率水平HIV/AIDS患者基本特征[n(%)]
Table 1. Basic characteristics of HIV/AIDS patients at different resting heart rate levels [n(%)]
特征 合计 静息心率 t/χ2/Z值 P值 正常(n=1 385) 过快(n=260) 年龄(岁) 49.1±12.3 49.7±12.2 46.0±11.9 21.06 < 0.001 性别 0.03 0.872 女 386(23.5) 326(84.5) 60(15.5) 男 1 259(76.5) 1 059(84.1) 200(15.9) 文化程度 15.31 < 0.001 小学及以下 713(43.3) 629(88.2) 84(11.8) 初中及以上 932(56.7) 756(81.1) 176(18.9) 腰围[M(P25, P75), cm] 83.0(77.5, 88.0) 83.0(78.0, 88.0) 82.1(76.3, 88.0) 1.14 0.285 臀围[M(P25, P75), cm] 92.7(89.0, 96.5) 93.0(89.0, 97.0) 92.0(87.1, 96.0) 5.62 0.018 腰臀比[M(P25, P75)] 0.9(0.8, 0.9) 0.9(0.8, 0.9) 0.9(0.8, 0.9) 0.59 0.442 腹部肥胖 2.00 0.158 否 781(47.5) 668(85.5) 113(14.5) 是 864(52.5) 717(83.0) 147(17.0) BMI[M(P25, P75), kg/m2] 22.2(20.4, 24.2) 22.3(20.4, 24.2) 21.9(20.2, 24.0) 2.28 0.131 BMI分组(kg/m2) 1.39 0.498 正常 1 060(64.4) 886(83.6) 174(16.4) 偏低 118(7.2) 98(83.1) 20(16.9) 偏高 467(28.4) 401(85.9) 66(14.1) 吸烟 16.32 < 0.001 否 939(57.1) 761(81.0) 178(19.0) 是 706(42.9) 624(88.4) 82(11.6) 饮酒 11.37 < 0.001 否 1 498(91.1) 1 247(83.2) 251(16.8) 是 147(8.9) 138(93.9) 9(6.1) 运动 1.47 0.225 否 1 159(70.5) 984(84.9) 175(15.1) 是 486(29.5) 401(82.5) 85(17.5) 正常高值血压 0.51 0.774 否 941(57.2) 796(84.6) 145(15.4) 是 704(42.8) 589(84.0) 115(16.0) 高血压 0.02 0.883 否 1 183(71.9) 997(84.3) 186(15.7) 是 462(28.1) 388(84.0) 74(16.0) 糖尿病 4.17 0.041 否 1 508(91.7) 1 278(84.7) 230(15.3) 是 137(8.3) 107(78.1) 30(21.9) TC[M(P25, P75), mmol/L] 4.6(4.1, 5.3) 4.7(4.1, 5.3) 4.6(4.0, 5.5) 0.00 0.955 TC分组(mmol/L) 0.14 0.712 < 6.2 1 509(91.7) 1 272(84.3) 237(15.7) ≥6.2 136(8.3) 113(83.1) 23(16.9) TG[M(P25, P75), mmol/L] 1.7(1.2, 2.6) 1.7(1.1, 2.5) 1.8(1.3, 3.0) 9.39 0.002 TG分组(mmol/L) 4.63 0.031 < 2.3 1 125(68.4) 962(85.5) 163(14.5) ≥2.3 520(31.6) 423(81.3) 97(18.7) LDL-C[M(P25, P75), mmol/L] 2.4(2.0, 2.9) 2.4(2.0, 2.9) 2.5(2.0, 2.9) 0.38 0.537 LDL-C分组(mmol/L) 1.92 0.165 < 4.1 1 592(96.8) 1 344(84.4) 248(15.6) ≥4.1 53(3.2) 41(77.4) 12(22.6) HDL-C[M(P25, P75), mmol/L] 1.0(0.9, 1.3) 1.0(0.9, 1.3) 1.0(0.8, 1.2) 7.31 0.007 HDL-C分组(mmol/L) 4.24 0.039 < 1.0 733(44.6) 602(82.1) 131(17.9) ≥1.0 912(55.4) 783(85.9) 129(14.1) 血脂异常 6.17 0.013 否 671(40.8) 583(86.9) 88(13.1) 是 974(59.2) 802(82.3) 172(17.6) 基线CD4+T淋巴细胞计数(个/μl) 0.02 0.883 < 350 765(46.5) 643(84.1) 122(15.9) ≥350 880(53.5) 742(84.3) 138(15.7) 注:对于分类变量,括号外为例数,括号内为构成比;对于不符合正态分布的连续型变量,括号外为中位数,括号内为四分位数。  下载: 导出CSV
下载: 导出CSV
表 2 静息心率与高血压和正常高值血压的关联分析
Table 2. Analysis of resting heart rate with hypertension and prehypertension
模型 RHR(次/min) 正常(n=1 385) 过快(n=260) 模型1 高血压比正常血压 1.00 1.49(1.01~2.20) a 正常高值血压比正常血压 1.00 1.24(0.89~1.73) 模型2 高血压比正常血压 1.00 1.45(0.98~2.14) b 正常高值血压比正常血压 1.00 1.21(0.87~1.69) 模型3 高血压比正常血压 1.00 1.02(1.01~1.03) c 正常高值血压比正常血压 1.00 1.01(1.00~1.02) a 模型4 高血压比正常血压 1.00 1.02(1.01~1.03) c 正常高值血压比正常血压 1.00 1.01(1.00~1.02) b 注:a P < 0.05; b P < 0.1; c P < 0.01;模型1和模型3校正的因素有年龄、性别、腹部肥胖、BMI,RHR作为分类变量纳入;模型2和模型4校正的因素有年龄、性别、腹部肥胖、BMI、TC、TG,RHR作为连续型变量纳入。
下载: 导出CSV
表 3 脂质与静息心率相乘交互作用探索
Table 3. Interactions between lipids and resting heart rate
变量 正常高值血压 高血压 aOR(95% CI)值 P值 aOR(95% CI)值 P值 TC×RHR 0.74(0.21~2.59) 0.637 0.69(0.18~2.71) 0.598 TG×RHR 0.43(0.21~0.86) 0.017 0.42(0.19~0.93) 0.032 LDL-C×RHR 0.41(0.06~2.66) 0.353 0.84(0.14~4.91) 0.843 HDL-C×RHR 1.85(0.95~3.60) 0.072 1.56(0.72~3.37) 0.261 注:多因素模型均校正了年龄、性别、BMI、腰臀比。
下载: 导出CSV
表 4 不同静息心率水平不同TG的HIV/AIDS患者正常高值血压和高血压患病情况
Table 4. Prevalence of prehypertension and hypertension in HIV / AIDS patients with different triglycerides at different resting heart rate levels
TG(mmol/L) RHR正常 RHR过快 人数 正常高值 高血压 人数 正常高值 高血压 < 2.3 962 395(41.1) 239(24.8) 163 75(46.0) 49(30.1) ≥2.3 423 194(45.9) 149(35.2) 97 40(41.2) 29(29.9) 合计 1 125 589(52.3) 388(34.5) 260 115(44.2) 78(30.0)
下载: 导出CSV
-
[1] Gallant J, Hsue PY, Shreay S, et al. Comorbidities among US patients with prevalent HIV infection-a trend analysis[J]. J Infect Dis, 2017, 216(12): 1525-1533. DOI: 10.1093/infdis/jix518. [2] Bauer S, Mwanza MW, Chilengi R, et al. Awareness and management of elevated blood pressure among human immunodeficiency virus-infected adults receiving antiretroviral therapy in urban Zambia: a call to action[J]. Glob Health Action, 2017, 10(1): 1359923. DOI: 10.1080/16549716.2017.1359923. [3] Calcagno A, Piconi S, Focà E, et al. Role of normalized T-Cell subsets in predicting comorbidities in a large cohort of geriatric HIV-infected patients[J]. J Acquir Immune Defic Syndr, 2017, 76(3): 338-342. DOI: 10.1097/QAI.0000000000001496. [4] 余燕云. 艾滋病抗病毒治疗者高血压患病及影响因素研究[D]. 昆明: 昆明医科大学, 2018.Yu YY. Prevalence of hypertension and associated factors among AIDS patients with antiviral therapy[D]. Kunming: Kunming Medical University, 2018. [5] Fahme SA, Bloomfield GS, Peck R. Hypertension in HIV-Infected adults novel pathophysiologic mechanisms[J]. Hypertension, 2018, 72(1): 44-55. DOI: 10.1161/HYPERTENSIONAHA.118.10893. [6] Kemal A, Teshome MS, Ahmed M, et al. Dyslipidemia and associated factors among adult patients on antiretroviral therapy in Armed Force Comprehensive and Specialized Hospital, Addis Ababa, Ethiopia[J]. HIV AIDS, 2020, 12: 221-231. DOI: 10.2147/HIV.S252391. [7] He DM, Fan FF, Jia J, et al. Lipid profiles and the risk of new-onset hypertension in a Chinese community-based cohort[J]. Nutr Metab Cardiovasc Dis, 2021, 31(3): 911-920. DOI: 10.1016/j.numecd.2020.11.026. [8] DeLalio LJ, Sved AF, Sean D Stocker SD. Sympathetic nervous system contributions to hypertension: updates and therapeutic relevance[J]. Can J Cardiol, 2020, 36(5): 712-720. DOI: 10.1016/j.cjca.2020.03.003. [9] Böhm M, Reil JC, Deedwania P, et al. Resting heart rate: risk indicator and emerging risk factor in cardiovascular disease[J]. Am J Med, 2015, 128(3): 219-228. DOI: 10.1016/j.amjmed.2014.09.016. [10] Eikelis N, Lambert EA, Phillips S, et al. Muscle sympathetic nerve activity is associated with elements of the plasma lipidomic profile in young asian adults[J]. J Clin Endocrinol Metab, 2017, 102(6): 2059-2068. DOI: 10.1210/jc.2016-3738. [11] Nestel PJ, Khan AA, Straznicky NE, et al. Markers of sympathetic nervous system activity associate with complex plasma lipids in metabolic syndrome subjects[J]. Atherosclerosis, 2017, 256: 21-28. DOI: 10.1016/j.atherosclerosis.2016.11.032. [12] Li S, Guo B, Chen H, et al. The role of the triglyceride (triacylglycerol) glucose index in the development of cardiovascular events: a retrospective cohort analysis[J]. Sci Rep, 2019, 9(1): 7320. DOI: 10.1038/s41598-019-43776-5. [13] 中国高血压防治指南修订委员会, 高血压联盟(中国), 中华医学会心血管病学分会, 等. 中国高血压防治指南(2018年修订版)[J]. 中国心血管杂志, 2019, 24(1): 24-56. DOI: 10.3969/j.issn.1007-5410.2019.01.002.Writing Group of 2018 Chinese Guidelines for the Management of Hypertension, Chinese Hypertension League, Chinese Society of Cardiology, et al. 2018 Chinese guidelines for the management of hypertension[J]. Chin J Cardiovasc Med, 2019, 24(1): 24-56. DOI: 10.3969/j.issn.1007-5410.2019.01.002. [14] 诸骏仁, 高润霖, 赵水平, 等. 中国成人血脂异常防治指南(2016年修订版)[J]. 中华健康管理学杂志, 2017, 11(1): 7-28. DOI: 10.3760/cma.j.issn.1671-7368.2017.01.006.Zhu JR, Gao RL, Zhao SP, et al. 2016 Chinese guideline for the management of dyslipidemia in adults[J]. Chin J Health Management, 2017, 11(1): 7-28. DOI: 10.3760/cma.j.issn.1671-7368.2017.01.006. [15] Wallace LMK, Theou O, Godin J, et al. Investigation of frailty as a moderator of the relationship between neuropathology and dementia in Alzheimer's disease: a cross-sectional analysis of data from the Rush Memory and Aging Project[J]. Lancet Neurol, 2019, 18(2): 177-184. DOI: 10.1016/S1474-4422(18)30371-5. [16] 徐小慧, 单淑晴, 时允, 等. 云南省德宏州接受抗病毒治疗的HIV感染者高血压患病率及其影响因素[J]. 中国初级卫生保健, 2020, 34(4): 48-51. DOI: 10.3969/j.issn.1001-568X.2020.04.0015.Xu XH, Shan SQ, Shi Y, et al. Prevalence and associated factors of hypertension among HIV-infected individuals receiving combination antiretroviral therapy in Dehong Prefecture, Yunnan Province[J]. Chinese Primary Health Care, 2020, 34(4): 48-51. DOI: 10.3969/j.issn.1001-568X.2020.04.0015. [17] Shi YY, Zhou W, Liu XJ, et al. Resting heart rate and the risk of hypertension and heart failure: a dose-response meta-analysis of prospective studies[J]. J Hypertens, 2018, 36(5): 995-1004. DOI: 10.1097/HJH.0000000000001627. [18] Custodis F, Schirmer SH, Baumhäkel M, et al. Vascular pathophysiology in response to increased heart rate[J]. J Am Coll Cardiol, 2010, 56(24): 1973-1983. DOI: 10.1016/j.jacc.2010.09.014. [19] Ding Y, Zhu B, Lin H, et al. HIV infection and electrocardiogram abnormalities: baseline assessment from the CHART cohort[J]. Clin Microbiol Infect, 2020, 26(12): 1689. e1-e7. DOI: 10.1016/j.cmi.2020.03.005. [20] Duro M, Sarmento-Castro R, Almeida C, et al. Lipid profile changes by high activity anti-retroviral therapy[J]. Clin Biochem, 2013, 46(9): 740-744. DOI: 10.1016/j.clinbiochem.2012.12.017. [21] Nduka C, Sarki A, Uthman O, et al. Impact of antiretroviral therapy on serum lipoprotein levels and dyslipidemias: a systematic review and meta-analysis[J]. Int J Cardiol, 2015, 199: 307-318. DOI: 10.1016/j.ijcard.2015.07.052. [22] 肖江, 郜桂菊, 李鑫, 等. 高效抗逆转录病毒治疗对艾滋病患者机体代谢的影响[J]. 中华实验和临床感染病杂志(电子版), 2011, 5(2): 133-141. DOI: 10.3877/cma.j.issn.1674-1358.2011.02.002.Xiao J, Gao GJ, Li X, et al. Analysis on metabolic consequence in patients with HIV infection after highly active antiretrovirus therapy[J]. Chin J Exp Clin Infec Dis(Electronic Edition), 2011, 5(2): 133-141. DOI: 10.3877/cma.j.issn.1674-1358.2011.02.002. [23] Ekoru K, Young EH, Dillon DG, et al. HIV treatment is associated with a two-fold higher probability of raised triglycerides: pooled analyses in 21 023 individuals in sub-Saharan Africa[J]. Glob Health Epidemiol Genom, 2018, e3-e7. DOI: 10.1017/gheg.2018.7. [24] Oort SV, Beulens JWJ, Ballegooijen AJV, et al. Association of cardiovascular risk factors and lifestyle behaviors with hypertension: a mendelian randomization study[J]. Hypertension, 2020, 76(6): 1971-1979. DOI: 10.1161/HYPERTENSIONAHA.120.15761. [25] Kajikawa M, Maruhashi T, Matsumoto T, et al. Relationship between serum triglyceride levels and endothelial function in a large community-based study[J]. Atherosclerosis, 2016, 249: 70-75. DOI: 10.1016/j.atherosclerosis.2016.03.035. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 586
- HTML全文浏览量: 241
- PDF下载量: 68
- 被引次数: 0