

Analysis of survival and its related factors of HIV/AIDS patient in Luzhou, 2010-2019
-
摘要:
目的 分析四川省泸州市HIV/AIDS患者生存情况及其影响因素。 方法 选取2010―2019年泸州市报告的≥15岁HIV/AIDS患者, 采用寿命表法计算生存率,采用Kaplan-Meier法计算中位生存时间和绘制生存曲线,采用Cox比例风险回归模型分析生存时间的影响因素。 结果 共纳入研究对象12 274例,中位生存时间为87.35(95% CI: 86.22~88.49)个月,确诊后1、3、5、7和9年累积生存率分别为78%、73%、69%、66%和63%;多因素分析结果显示,在发生AIDS相关死亡风险方面,男性是女性的1.491倍;汉族是其他民族的2.118倍;离异或丧偶是已婚的1.545倍;确诊感染时的年龄≥60岁是15~<20岁的3.392倍;大专及以上是文盲的0.473倍;注射毒品、采(供)血及输血/血液制品是异性性传播的1.513倍;样本来源于医疗机构是检测咨询的1.131倍;首次检测CD4+T淋巴细胞计数为≥501个/μl是≤200个/μl的0.205倍;首次诊断疾病状态为AIDS是HIV感染的1.166倍;未接受抗病毒治疗是接受抗病毒治疗的3.524倍。 结论 性别、婚姻状况、诊断时的年龄、文化程度、感染途径、样本来源、首次检测CD4+T淋巴细胞计数、疾病状态及抗病毒治疗是影响HIV/AIDS患者生存时间的因素,早发现、早诊断、早治疗可降低HIV/AIDS患者的死亡风险。 -
关键词:
- HIV/AIDS患者 /
- 生存时间 /
- 影响因素
Abstract:Objective To analyze the survival of HIV/AIDS patient and its related factors in Luzhou City. Methods The HIV/AIDS patient aged 15 years and above in Luzhou City from 2010 to 2019 were selected. Life table method was used to calculate the survival rate. Kaplan-Meier method was used to calculate the average survival time and draw the survival curve. Cox proportion hazard regression model was performed to identify the factors related to survival time. Results A total number of 12 274 cases were selected, the median survival time was 87.35 (86.22-88.49) months. The survival rate of 1, 3, 5, 7 and 9 years were 78%, 73%, 69%, 66%, and 63% respectively. Cox multivariate analysis showed that the risk of death in men was 1.491 times that than in women. The Han had 2.118 the risk times than other ethnic groups. The divorced or widowed had 1.545 times the risk than the married. The aged 60 years and above at the time of infection had 3.392 times risk than the aged less than or equal to 15- < 21 years old. The college and above had 0.473 the risk times than the illiteracy. Injecting drugs, collecting (supplying) blood and blood/blood products transfusions were 1.513 times than heterosexual transmission. The samples obtained from medical institutions were 1.131 times than detection of consulting. The first CD4+T cell test value of 501- cells/μl was 0.205 times than ≤200 cells/μl. First diagnosed AIDS was 1.166 times than HIV infection. Not receiving antiviral treatment was 3.524 times than receiving antiviral treatment. Conclusions The factors such as gender, marital status, age, education level, transmission route, sample source, first CD4+T cell count, disease state and antiviral treatment affect the survival of HIV/AIDSpatient. Early detection, early diagnosis, and early treatment can reduce the risk of death from HIV/AIDS cases. -
Key words:
- HIV/AIDS patient /
- Survival analysis /
- Influencing factors
-

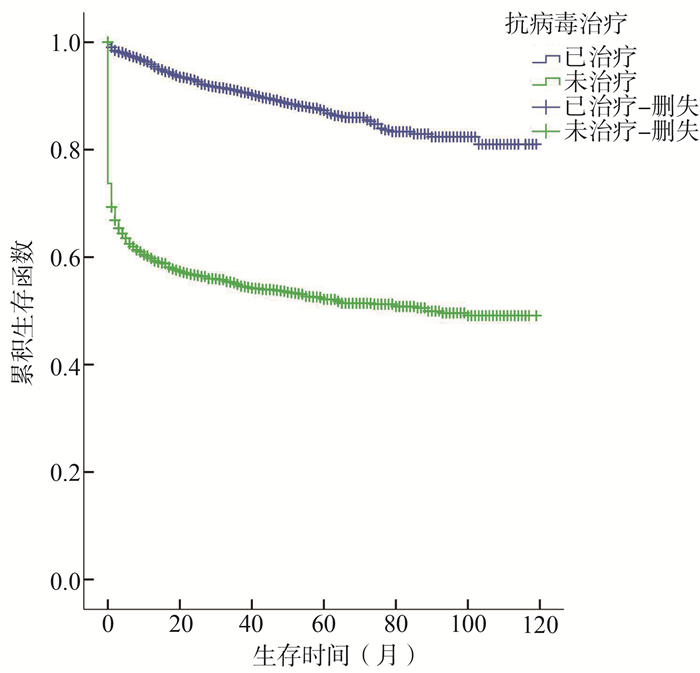
图 1 不同治疗情况的HIV/AIDS患者生存曲线
Figure 1. Survival curves of HIV/AIDS cases with different treatment situations

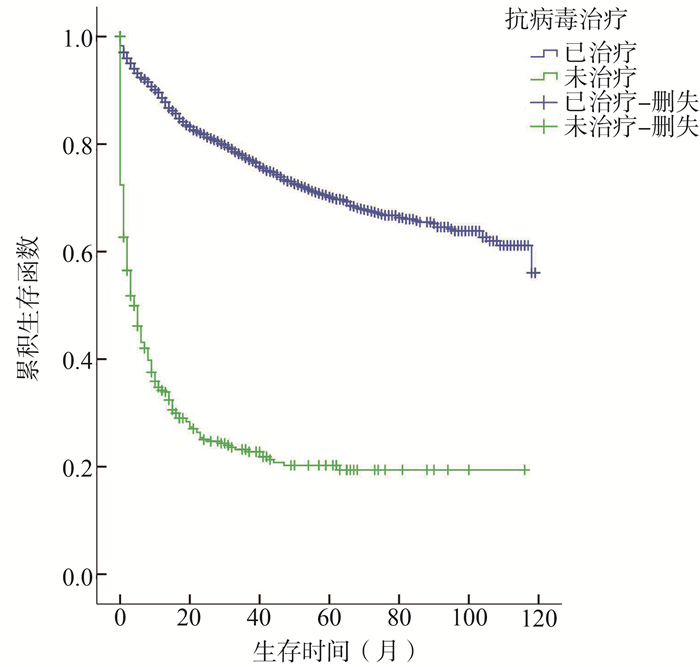
图 2 不同治疗情况的HIV感染者生存曲线
Figure 2. Survival curves of HIV infectors with different treatment situations

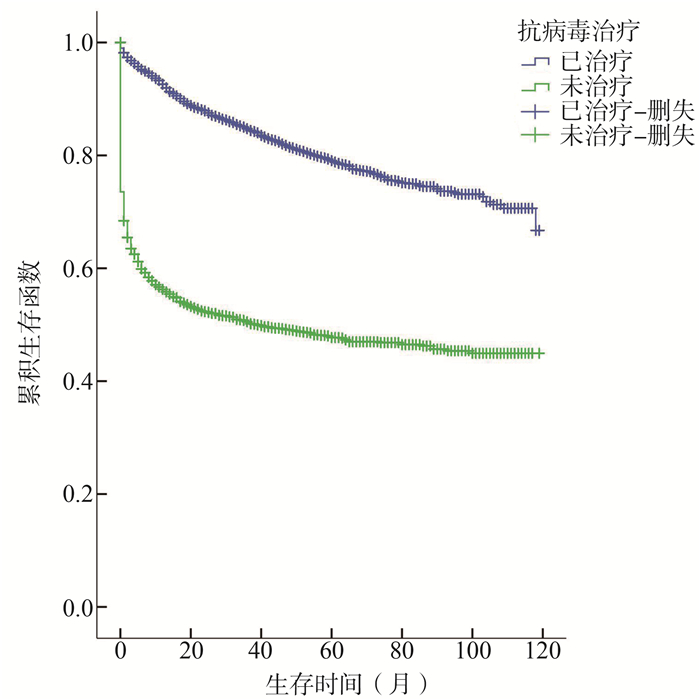
图 3 不同治疗情况的AIDS患者生存曲线
Figure 3. Survival curves of AIDS patients with different treatment situations
表 1 2010―2019年泸州市HIV/AIDS患者生存状况
Table 1. Survival situation of HIV/AIDS cases in Luzhou from 2010 to 2019
观察时间(月) 期初观察人数 删失人数 有效观察人数 死亡人数 死亡率 生存率 累积生存率 累积生存率标准误 0 12 274 3 070 10 739.0 1 800 0.17 0.83 0.83 0.00 12 7 404 2 107 6 350.5 375 0.06 0.94 0.78 0.00 24 4 922 1 221 4 311.5 147 0.03 0.97 0.76 0.00 36 3 554 953 3 077.5 113 0.04 0.96 0.73 0.01 48 2 488 768 2 104.0 59 0.03 0.97 0.71 0.01 60 1 661 498 1 412.0 39 0.03 0.97 0.69 0.01 72 1 124 433 907.5 21 0.02 0.98 0.67 0.01 84 670 263 538.5 12 0.02 0.98 0.66 0.01 96 395 207 291.5 6 0.02 0.98 0.64 0.01 ≥108 182 180 92.0 2 0.02 0.98 0.63 0.01  下载: 导出CSV
下载: 导出CSV
表 2 2010―2019年泸州市HIV/AIDS患者生存时间相关因素的Cox比例风险模型分析
Table 2. Cox proportional hazard regression model analyses with the HIV/AIDS cases in Luzhou from 2010 to 2019
变量 HIV/AIDS患者数(n=12 274) 死亡例数[n(%)] 单因素分析 多因素分析 HR(95% CI)值 P值 HR(95% CI)值 P值 性别 女 3 305(26.93) 455(17.68) 1.000 1.000 男 8 969(73.07) 2 119(82.32) 1.844(1.667~2.041) <0.001 1.491(1.342~1.656) <0.001 民族 其他 111(0.90) 9(0.35) 1.000 1.000 汉 12 163(99.10) 2 565(99.65) 2.632(1.368~5.065) 0.004 2.118(1.099~4.082) 0.025 婚姻状况 已婚 5 627(45.84) 963(37.41) 1.000 1.000 未婚 2 237(18.23) 431(16.74) 1.018(0.909~1.141) 0.753 1.605(1.416~1.820) <0.001 离异或丧偶 4 229(34.45) 1 169(45.42) 1.620(1.488~1.764) <0.001 1.545(1.415~1.687) <0.001 不详 181(1.47) 11(0.43) 0.227(0.125~0.411) <0.001 0.223(0.122~0.405) <0.001 确诊感染时的年龄组(岁) 15~<21 280(2.28) 21(0.82) 1.000 1.000 21~<41 2 708(22.06) 348(13.52) 1.877(1.208~2.916) 0.005 1.382(0.864~2.211) 0.177 41~<60 4 662(37.98) 874(33.95) 3.476(2.254~5.359) <0.001 2.181(1.358~3.502) 0.001 ≥60 4 624(37.67) 1 331(51.71) 6.702(4.351~10.323) <0.001 3.392(2.100~5.478) <0.001 职业 农民及民工 8 236(67.10) 1 915(74.40) 1.000 1.000 家政、家务及待业 2 199(17.92) 379(14.72) 0.625(0.559~0.698) <0.001 0.863(0.769~0.968) 0.012 离退人员 280(2.28) 90(3.50) 1.351(1.094~1.669) 0.005 0.997(0.799~1.244) 0.980 工人 312(2.54) 50(1.94) 0.557(0.420~0.738) <0.001 0.808(0.608~1.075) 0.143 商业服务 399(3.25) 38(1.48) 0.311(0.226~0.429) <0.001 0.859(0.617~1.196) 0.367 干部职员 73(0.59) 6(0.23) 0.248(0.111~0.552) 0.001 0.720(0.319~1.628) 0.430 学生 108(0.88) 4(0.16) 0.114(0.043~0.305) <0.001 0.486(0.171~1.387) 0.178 其他及不详 667(5.43) 92(3.57) 0.427(0.346~0.527) <0.001 0.613(0.493~0.763) <0.001 文化程度a 文盲 1 699(13.84) 520(20.20) 1.000 1.000 小学 5 680(46.28) 1 276(49.57) 0.661(0.597~0.732) <0.001 0.846(0.761~0.941) 0.002 中学 4 208(34.28) 732(28.44) 0.409(0.365~0.458) <0.001 0.740(0.648~0.846) <0.001 大专及以上 656(5.34) 46(1.79) 0.149(0.110~0.201) <0.001 0.473(0.340~0.657) <0.001 感染途径 异性性传播 11 064(90.14) 2 476(96.19) 1.000 1.000 同性性传播 805(6.56) 66(2.56) 0.284(0.222~0.363) <0.001 0.656(0.504~0.853) 0.002 注射毒品、采(供)血及输血/血液制品 100(0.81) 29(1.13) 0.959(0.665~1.383) 0.822 1.513(1.009~2.270) 0.045 其他及不详 305(2.48) 3(0.12) 0.031(0.010~0.096) <0.001 0.020(0.006~0.061) <0.001 样本来源 检测咨询 1 868(15.22) 307(11.93) 1.000 1.000 医疗机构 8 681(70.73) 2 029(78.83) 1.703(1.510~1.920) <0.001 1.131(1.001~1.278) 0.049 羁押场所 196(1.60) 34(1.32) 1.028(0.722~1.465) 0.878 0.665(0.451~0.981) 0.040 其他 1 529(12.46) 204(7.92) 1.277(1.069~1.527) 0.007 0.886(0.739~1.063) 0.192 首次检测CD4+T淋巴细胞计数(个/μl) ≤200 2 167(17.66) 811(31.51) 1.000 1.000 201~350 2 869(23.37) 299(11.62) 0.240(0.210~0.274) <0.001 0.309(0.265~0.360) <0.001 351~500 2 335(19.02) 177(6.88) 0.165(0.140~0.194) <0.001 0.242(0.200~0.293) <0.001 ≥501 2 440(19.88) 143(5.55) 0.117(0.098~0.140) <0.001 0.205(0.166~0.254) <0.001 未检测 2 463(20.07) 1 144(44.44) 1.252(1.143~1.371) <0.001 0.870(0.731~1.036) 0.118 首次诊断疾病状态 HIV 7 665(62.45) 1 490(57.89) 1.000 1.000 AIDS 4 609(37.55) 1 084(42.11) 1.210(1.119~1.309) <0.001 1.166(1.015~1.339) 0.030 抗病毒治疗 是 9 371(76.35) 1 156(44.91) 1.000 1.000 否 2 903(23.65) 1 418(55.09) 4.561(4.219~4.931) <0.001 3.524(3.107~3.997) <0.001 注:a HIV/AIDS患者数有部分缺失。
下载: 导出CSV
-
[1] Lee LM, Karon JM, Selik R, et al. Survival after AIDS diagnosis in adolescents and adults during the treatment era, United States, 1984-1997[J]. JAMA, 2001, 285(10): 1308-1315. DOI: 10.1001/jama.285.10.1308. [2] 陈婧, 徐敏, 赵啸, 等. 北京市2005-2015年艾滋病抗病毒治疗患者生存及其影响因素[J]. 中华疾病控制杂志, 2018, 22(12): 1225-1228. DOI: 10.16462/j.cnki.zhjbkz.2018.12.006.Chen J, Xu M, Zhao X, et al. Analysis of the survival conditions of HIV/AIDS patients receiving antiretroviral therapy in Beijing in 2005-2015 and the related factors[J]. Chin J Dis Control Prev, 2018, 22(12): 1225-1228. DOI: 10.16462/j.cnki.zhjbkz.2018.12.006. [3] 许文平, 邹家凤, 余明, 等. 1996-2016年泸州市艾滋病患者人群特征分析[J]. 应用预防医学, 2018, 24(3): 210-211. DOI: 10.3969/j.issn.1673-758X.2018.03.013.Xu WP, Zhou JF, Yu M, et al. Analysis of epidemiological characteristics of AIDS patients in Luzhou city from 1996 to 2016[J]. Applied Prev Med, 2018, 24(3): 210-211. DOI: 10.3969/j.issn.1673-758X.2018.03.013. [4] 冯瑞芳, 刘中夫. HIV感染者/AIDS病人死亡原因的研究进展[J]. 中国艾滋病性病, 2013, 19(3): 229-231. DOI: 10.13419/j.cnki.aids.2013.03.027.Feng RF, Liu ZF. Analysis of the causes of death of HIV infectors/AIDS patients[J]. Chin J AIDS STD, 2013, 19(3): 229-231. DOI: 10.13419/j.cnki.aids.2013.03.027. [5] 邓玲, 刘中夫, 张石则, 等. 四川省凉山州2008-2013年艾滋病患者生存时间及影响因素分析[J]. 中华流行病学杂志, 2015, 36(6): 569-575. DOI: 103760/cma.j.issn.0254-6450.2015.06.007.Deng L, Liu ZF, Zhang SZ, et al. Survival time and related influencing factors of AIDS patients in Liangshan prefecture, Sichuan province, during 2008-2013[J]. Chin J Epidemiol, 2015, 36(6): 569-575. DOI: 103760/cma.j.issn.0254-6450.2015.06.007. [6] 葛锐, 胡洁, 张倩倩, 等. 嘉兴市HIV/AIDS病人生存时间及影响因素分析[J]. 中国艾滋病性病, 2018, 24(10): 1001-1003. DOI: 10.13419/j.cnki.aids.2018.10.11.Ge R, Hu J, Zhang QQ, et al. Survival time of HIV/AIDS patients and influencing factors in Jiaxing[J]. Chin J AIDS STD, 2018, 24(10): 1001-1003. DOI: 10.13419/j.cnki.aids.2018.10.11. [7] 李洋, 王娟, 贺淑芳, 等. 北京市1995-2015年艾滋病病例诊断后生存时间与影响因素分析[J]. 中华流行病学杂志, 2017, 38(11): 1509-1513. DOI: 103760/cma.j.issn.0254-6450.2017.11.014.Li Y, Wang J, He SF, et al. Survival time of HIV/AIDS cases and related factors in Beijing, 1995―2015[J]. Chin J Epidemiol, 2017, 38(11): 1509-1513. DOI: 103760/cma.j.issn.0254-6450.2017.11.014. [8] Li M, Tang W, Bu K, et al. Mortality among People Living with HIV and AIDS in China: Implications for Enhancing Linkage[J]. Sci Rep, 2016, 6: 28005. DOI: 10.1038/srep28005. [9] Antiretroviral Therapy Cohort Collaboration. Survival of HIV-positive patients starting antiretroviral therapy between 1996 and 2013: a collaborative analysis of cohort studies[J]. Lancet HIV, 2017, 4(8): e349-e356. DOI: 10.1016/S2352-3018(17)30066-8. [10] 罗映娟, 喻航, 黄俊, 等. 四川省艾滋病抗病毒治疗现状分析[J]. 预防医学情报杂志, 2015, 31(1): 51-53. DOI: CNKI:SUN:YFYX.0.2015-01-013.Luo YJ, Yu H, Huang J, et al. Status of antiviral therapy for HIV/AIDS in Sichuan[J]. J Prev Med Inf, 2015, 31(1): 51-53. DOI: CNKI:SUN:YFYX.0.2015-01-013. [11] 过恒升, 冯献湘, 章奇, 等. 柳州市2008-2018年HIV/AIDS生存状况及影响因素分析[J]. 中华流行病学杂志, 2020, 41(12): 2098-2103. DOI: 10.3760/cma.j.cn112338-20200228-00211.Guo HS, Feng XX, Zhang Q, et al. Survival status and influencing factors of HIV/AIDS cases in Liuzhou, 2008―2018[J]. Chin J Epidemiol, 2020, 41(12): 2098-2103. DOI: 10.3760/cma.j.cn112338-20200228-00211. [12] 周琳, 吴琼海, 沈伟伟, 等. 浙江省台州市接受抗病毒治疗的艾滋病患者生存分析[J]. 中华疾病控制杂志, 2013, 17(12): 1049-1051. DOI: CNKI:SUN:JBKZ.0.2013-12-012.Zhou L, Wu QH, Shen WW, et al. Survival analysis of HIV/AIDS patients receiving a ntiretroviral treatment in Taizhou City of Zhejiang province, China[J]. Chin J Dis Control Prev, 2013, 17(12): 1049-1051. DOI: CNKI:SUN:JBKZ.0.2013-12-012. [13] 刘雪梅, 过恒升, 范引光, 等. 广西柳州MSM艾滋病非职业性暴露后预防服务的需求和影响因素[J]. 中华疾病控制杂志, 2019, 23(12): 1517-1522. DOI: 10.16462/j.cnki.zhjbkz.2019.12.016.Liu XM, Guo HS, Fan YG, et al. Demand for non-occupational post-exposure prophylaxis services for HIV and associated factors a-mong men who have sex with men in Liuzhou, Guangxi[J]. Chin J Dis Control Prev, 2019, 23(12): 1517-1522. DOI: 10.16462/j.cnki.zhjbkz.2019.12.016. [14] Park IU, Chow JM, Bolan G, et al. Screening for syphilis with the treponemal immunoassay: analysis of discordant serology results and implications for clinical management[J]. J Infect Dis, 2011, 204(9): 1297-1304. DOI: 10.1093/infdis/jir524. [15] Larsen SA, Steiner BM, Rudolph AH. Laboratory diagnosis and interpretation of tests for syphilis[J]. Clin Microbiol Rev, 1995, 8(1): 1-21. DOI: 10.1128/CMR.8.1.1-21. [16] Zhang F, Dou Z, Ma Y, et al. Effect of earlier initiation of antiretroviral treatment and increased treatment coverage on HIV-related mortality in China: a national observational cohort study[J]. Lancet Infect Dis, 2011, 11(7): 516-524. DOI: 10.1016/S1473-3099(11)70097-4. [17] 孙丽, 周建波. 江苏省某市HIV/AIDS患者死亡病例生存时间的影响因素及其交互作用分析[J]. 中国皮肤性病学杂志, 2017, 31(12): 1327-1329, 1352. DOI: 10.13735/j.cjdv.1001-7089.201703172.Sun L, Zhou JB. Analysis of influencing factors of survival time and their interaction in HIV/AIDS death cases in a city of Jiangsu province[J]. Chin J Derm Venereol, 2017, 31(12): 1327-1329, 1352. DOI: 10.13735/j.cjdv.1001-7089.201703172. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 519
- HTML全文浏览量: 326
- PDF下载量: 65
- 被引次数: 0