

Association between short-term air pollution exposure and placental abruption: a nested case-control study
-
摘要:
目的 探索大气污染短期暴露与胎盘早剥发病风险的关联。 方法 采用巢式病例对照研究,以重庆市大型出生队列2018年7月31日—2022年7月31日新发798例胎盘早剥孕妇作为病例组,按照年龄、孕周、孕次、产次和分娩日期的匹配因素以1∶4的比例匹配,匹配未发生胎盘早剥的对照组3 192例。通过机器学习算法估算研究期间6种空气污染物(PM10、PM2.5、NO2、CO、O3和SO2)及气象因素数据集,并与每位研究对象居住地址的经纬度匹配。构建基于条件logistic回归的分布滞后非线性模型探索大气污染物短期暴露与胎盘早剥的暴露-反应关系,控制环境温度、相对湿度、风速、大气压力和归一化差异植被指数,以及孕妇年龄、孕周、孕次、产次、分娩季节、是否经历疫情、家庭住址的影响。 结果 单污染物模型结果显示,累积暴露4~7 d内,NO2与胎盘早剥发病风险升高存在显著关联,NO2每四分位数间距增加对应的OR值及95% CI为1.38(95% CI: 1.11~1.73, P<0.001)~1.54(95% CI: 1.18~2.02, P<0.001)。总体剂量-反应关系曲线显示,随着NO2浓度升高,胎盘早剥发病风险增加,暴露-反应曲线近似呈线性,其他污染物短期暴露与胎盘早剥风险的关联均无统计学意义(均P>0.05)。 结论 NO2短期暴露与胎盘早剥急性发病风险升高存在关联,可能是胎盘早剥的影响因素,未来有必要对此进一步开展研究加以验证。 Abstract:Objective To explore the association between short-term air pollution exposure and acute onset of placental abruption. Methods This study is a nested case-control study nested in the large birth cohort of Chongqing. A total of 798 pregnant women with new placental abruption from July 31, 2018 to July 31, 2022 were selected as the case group. A control group of 3, 192 women without abruptio placentae was matched at a ratio of 1∶4 according to age, gestational age, gravidity, parity, and delivery date. The data set of six air pollutants (PM10, PM2.5, NO2, CO, O3, SO2) and meteorological factors was estimated by machine learning algorithm and matched with the longitude and latitude of each subject′s residence address. A distributed lag non-linear models based on conditional Logistic regression was constructed to explore the exposure-response relationship between short-term air pollutants exposure and placental abruption, controlling the effects of temperature, relative humidity, wind speed, atmospheric pressures and NDVI, as well as the age, gestation week, gravidity (first pregnancy/non-first pregnancy), pravity (first birth/non-first birth), delivery season (cool/warm seasons), whether experienced the epidemic (Yes/No), and residential address (urban/countryside). Results The results of single pollutant model showed that NO2 was significantly associated with the increased risk of placental abruption within 4 to 7 days of cumulative exposure, and the odds ratio for each increase in IQR of NO2 was 1.38 (95% CI: 1.11-1.73, P < 0.001) to to 1.54 (95% CI: 1.18-2.02, P < 0.001). The overall dose-response curve showed that the risk of placental abruption increased with the increase of NO2 concentration, and the exposure-response curve was approximately linear. There was no statistically significant association between short-term exposure to other pollutants and the risk of placental abruption. Conclusions Short-term exposure to NO2 is associated with an increased risk of acute onset of placental abruption, which may be an influencing factor of placental abruption, and further studies are necessary to verify this. -
Key words:
- Air pollutants /
- Placental abruption /
- Distributed lag non-linear model
-

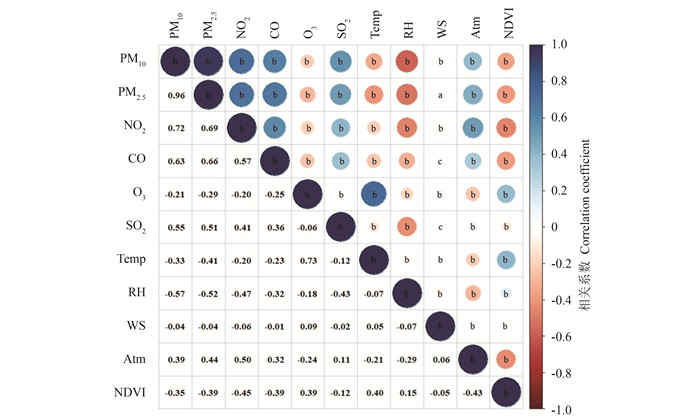
图 1 大气污染物与气象因素Spearman相关性热图
Temp: 环境温度;RH: 相对湿度;WS: 风速;Atm: 大气压力;NDVI: 归一化差异植被指数。
a: P<0.05;b: P<0.01。Figure 1. Heat map of Spearman correlation between air pollutants and meteorological factors
Temp: temperature; RH: relative humidity; WS: wind speed; Atm: atmospheric pressure; NDVI: normalized difference vegetation index.
a: P < 0.05;b: P < 0.01.
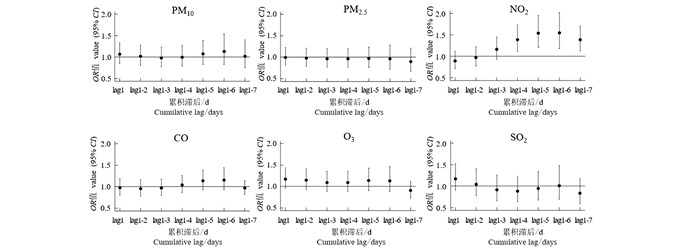
图 2 不同累积滞后时空气污染物与胎盘早剥的关联
通过分布滞后非线性模型进行估计,调整了环境温度、相对湿度、风速、大气压力和归一化差异植被指数,以及年龄、孕周、孕次、产次、家庭住址,是否经历疫情和分娩季节。计算空气污染物每IQR升高对应的OR值及95% CI。
Figure 2. Association between lag cumulative exposure of air pollutants and placental abruption
Estimated by the distributed lag non-linear model, adjusted for ambient temperature, relative humidity, weed speed, atmospheric pressure, and normalized difference vegetation index; as well as age, gestational weeks, gravidity, parity, residential address, whether experienced the epidemic, and delivery season. The ORs and 95% CI were calculated for each IQR increase in each air pollutants.

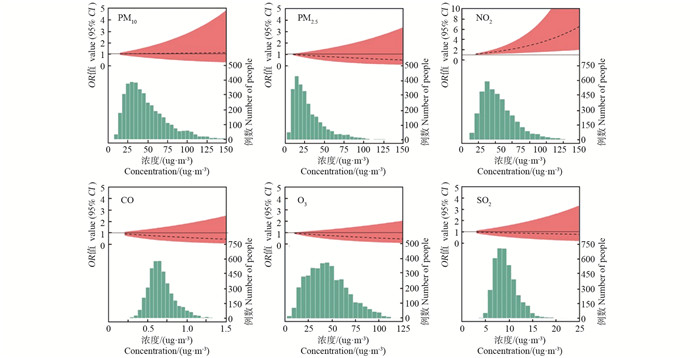
图 3 大气污染物与胎盘早剥风险总体剂量-反应关系图
通过分布滞后非线性模型进行估计,调整了环境温度、相对湿度、风速、大气压力和归一化差异植被指数,以及年龄、孕周、孕次、产次、家庭住址,是否经历疫情及分娩季节。
Figure 3. Overall dose-response relationship between air pollutants and the risk of placental abruption
Estimated by the distributed lag non-linear model, adjusted for ambient temperature, relative humidity, weed speed, atmospheric pressure, and normalized difference vegetation index; as well as age, gestational weeks, gravidity, parity, residential address, whether experienced the epidemic, and delivery season.
表 1 一般人口学特征与环境因素分布
Table 1. Distribution of demographic characteristics and environmental factors
变量 Variable 对照组 ② Control group ②
(n=3 192)病例组 ② Case group ②
(n=798)P值
value ③年龄/岁 Age/years 29.4±4.4 29.6±4.5 0.217 孕周/周 Gestational week/weeks 37.9±2.1 37.3±2.3 < 0.001 出生身长/cm Birth length/cm 49.1±2.4 48.5±2.8 < 0.001 出生体重/g Birth weight/g 3 119.5±547.1 2 941.2±576.6 < 0.001 孕次 Gravidity < 0.001 初孕 First pregnancy 899(28.2) 322(40.4) 非初孕 Non-first pregnancy 2 293(71.8) 476(59.6) 产次 Pravity < 0.001 初产 First birth 1 458(45.7) 498(62.4) 非初产 Non-first birth 1 734(54.3) 300(37.6) 经历疫情 Whether experienced the epidemic 0.609 否 Yes 1 151(36.1) 280(35.1) 是 No 2 041(63.9) 518(64.9) 出生季节 ① Delivery season① 0.474 暖季 Warm seasons 1 777(55.7) 433(54.3) 冷季 Cool seasons 1 415(44.3) 365(45.7) 家庭住址 Residential address < 0.001 主城区 Urban 1 150(36.0) 494(61.9) 区县 Countryside 2 042(64.0) 304(38.1) 患有 HDP Whether had HDP 0.287 是 Yes 199(6.2) 58(7.3) 否 No 2 993(93.8) 740(92.7) 环境因素 Environmental factors PM10/(g·m-3) 48.0±26.4 50.5±27.6 0.012 PM2.5/(g·m-3) 30.0±20.4 31.9±21.8 0.025 NO2/(g·m-3) 21.3±9.8 24.5±11.2 < 0.001 CO/(mg·m-3) 0.7±0.2 0.7±0.2 0.077 O3/(g·m-3) 45.8±21.1 46.3±22.8 0.940 SO2/(g·m-3) 9.3±2.4 9.3±2.5 0.154 温度/℃ Temperature/℃ 18.1±7.3 18.7±7.3 0.029 相对湿度/% Relative humidity/% 74.8±12.3 73.0±12.7 < 0.001 风速/(m·s-1) Wind speed/(m·s-1) 1.1±0.7 1.1±0.7 0.044 气压/hpa Air pressure/hpa 952.7±26.2 962.5±18.2 < 0.001 NDVI 3 701.3±1 713.4 3 427.9±1 587.3 < 0.001 注:HDP,妊娠期高血压疾病;NDVI,归一化差异植被指数。
①暖季:5—10月,冷季:11—次年4月;②以人数(占比%)或x±s表示;③使用Wilcoxon检验或χ2检验比较组间差异,P < 0.05为差异有统计学意义。
Note: HDP, hypertensive disorders of pregnancy; NDVI, normalized difference vegetation index.
① Warm season: May-October, cold season: November-April of the following year; ② Number of people(proportion/%) or x±s; ③Differences between two groups were compared using the Wilcoxon test or the chi-square test. P < 0.05 indicates statistically significant. 下载: 导出CSV
下载: 导出CSV
表 2 敏感性分析
Table 2. Sensitivity analysis
大气污染
Air pollution双污染物模型 ① Dual-pollution model① PM10 PM2.5 NO2 CO O3 SO2 PM10 — 1.77(0.89~3.50) 0.75(0.53~1.08) 1.09(0.78~1.52) 1.05(0.77~1.44) 1.06(0.76~1.47) PM2.5 0.57(0.30~1.08) — 0.70(0.51~0.97) 0.93(0.68~1.28) 0.91(0.67~1.22) 0.92(0.68~1.26) NO2 1.55(1.23~1.97) 1.56(1.24~1.95) — 1.49(1.20~1.86) 1.38(1.12~1.70) 1.41(1.14~1.73) CO 0.88(0.70~1.11) 0.91(0.72~1.15) 0.80(0.64~1.01) — 0.90(0.73~1.12) 0.92(0.74~1.14) O3 0.83(0.59~1.18) 0.84(0.59~1.19) 0.90(0.63~1.29) 0.87(0.61~1.23) — 0.84(0.59~1.19) SO2 0.96(0.81~1.15) 0.98(0.83~1.16) 0.93(0.79~1.11) 0.98(0.83~1.17) 0.98(0.83~1.16) — 大气污染
Air pollution去除匹配变量 ②
Remove the match variable ②单因素模型 ③
Single factor model ③额外调整HDP ④
Additional adjustment HDP ④PM10 1.05(0.77~1.43) 2.23(1.75~2.85) 1.02(0.74~1.39) PM2.5 0.92(0.69~1.24) 2.00(1.58~2.52) 0.89(0.66~1.20) NO2 1.41(1.15~1.71) 2.28(1.98~2.64) 1.38(1.12~1.70) CO 0.88(0.71~1.08) 1.27(1.07~1.51) 0.90(0.73~1.12) O3 0.82(0.59~1.15) 1.08(0.80~1.45) 0.84(0.59~1.19) SO2 0.94(0.81~1.11) 0.91(0.79~1.05) 0.97(0.82~1.15) 注:1. HDP,妊娠期高血压疾病。
2. 通过分布滞后非线性模型进行估计,计算空气污染物每IQR升高对应的OR值及95% CI。
3. “—”表示无数据。
①双污染物模型中每次额外纳入另一种污染物进行分析; ②在去除匹配变量模型中调整了环境温度、相对湿度、风速、大气压力和归一化差异植被指数,以及家庭住址,是否经历疫情和分娩季节; ③单因素模型中未调整任何协变量; ④额外纳入HDP进行调整。
Note: 1. HDP, hypertensive disorders of pregnancy.
2. Estimated by the distributed lag non-linear model, OR and 95% CI were calculated for each IQR increase in each air pollutants.
3. "—" indicates no date available.
①Another pollutant is additionally included for analysis each time in the dual-pollutant model; ② Temperature, relative humidity, wind speed, atmospheric pressure and normalized difference vegetation index, as well as residential address, whether experienced the epidemic and delivery season were adjusted in the model of removing variables; ③ No covariates were adjusted in the univariate model; ④ Additional adjustment of HDP.
下载: 导出CSV
-
[1] Brandt JS, Ananth CV. Placental abruption at near-term and term gestations: pathophysiology, epidemiology, diagnosis, and management[J]. Am J Obstet Gynecol, 2023, 228(5S): S1313-S1329. DOI: 10.1016/j.ajog.2022.06.059. [2] Downes KL, Grantz KL, Shenassa ED. Maternal, labor, delivery, and perinatal outcomes associated with placental abruption: a systematic review[J]. Am J Perinatol, 2017, 34(10): 935-957. DOI: 10.1055/s-0037-1599149. [3] Riihimäki O, Metsäranta M, Paavonen J, et al. Placental abruption and child mortality[J]. Pediatrics, 2018, 142(2): e20173915. DOI: 10.1542/peds.2017-3915. [4] 林琳, 陈艳红, 杜丽丽, 等. 单胎妊娠发生胎盘早剥的危险因素及母儿结局分析: ——一项9年的回顾性临床研究[J]. 中国妇幼健康研究, 2020, 31(12): 1585-1591. DOI: 10.3969/j.issn.1673-5293.2020.012.001.Lin L, Chen YH, Du LL, et al. Risk factors of placental abruption in singleton pregnancy and maternal-fetal outcomes—a 9-year retrospective study[J]. Chinese Journal of Woman and Child Health Research, 2020, 31(12): 1585-1591. DOI: 10.3969/j.issn.1673-5293.2020.012.001. [5] Oyelese, Ananth CV. Placental abruption[J]. Obstet Gynecol, 2006, 108(4): 1005-1016. DOI: 10.1097/01.aog.0000239439.04364.9a. [6] Tikkanen M. Placental abruption: epidemiology, risk factors and consequences[J]. Acta Obstet Gynecol Scand, 2011, 90(2): 140-149. DOI: 10.1111/j.1600-0412.2010.01030.x [7] Schifano P, Asta F, Dadvand P, et al. Heat and air pollution exposure as triggers of delivery: a survival analysis of population-based pregnancy cohorts in Rome and Barcelona[J]. Environ Int, 2016, 88: 153-159. DOI: 10.1016/j.envint.2015.12.013. [8] Darrow LA, Klein M, Flanders WD, et al. Ambient air pollution and preterm birth: a time-series analysis[J]. Epidemiology (Cambridge, Mass), 2009, 20(5): 689-698. DOI: 10.1097/EDE.0b013e3181a7128f. [9] Ming X, He ZY, Li YN, et al. The short-term effects of air pollution exposure on preterm births in Chongqing, China: 2015-2020[J]. Environ Sci Pollut Res Int, 2023, 30(18): 51679-51691. DOI: 10.1007/s11356-023-25624-2. [10] Xiao H, Yao CY, Qi ZL, et al. Association between maternal short-term exposure to ambient air pollution and the risk of fetal distress: A matched case-control study[J]. Sci Total Environ, 2023, 860: 160438. DOI: 10.1016/j.scitotenv.2022.160438. [11] Ananth CV, Kioumourtzoglou MA, Huang YM, et al. Exposures to air pollution and risk of acute-onset placental abruption: a case-crossover study[J]. Epidemiology (Cambridge, Mass), 2018, 29(5): 631-638. DOI: 10.1097/EDE.0000000000000859. [12] Michikawa T, Morokuma S, Yamazaki S, et al. Air pollutant exposure within a few days of delivery and placental abruption in Japan[J]. Epidemiology (Cambridge, Mass), 2017, 28(2): 190-196. DOI: 10.1097/EDE.0000000000000605. [13] Zhou WZ, Ming X, Yang YP, et al. Association between maternal exposure to ambient air pollution and the risk of preterm birth: a birth cohort study in Chongqing, China, 2015-2020[J]. Int J Environ Res Public Health, 2022, 19(4): 2211. DOI: 10.3390/ijerph19042211. [14] Mi T, Tang D, Fu JB, et al. Data augmentation for bias correction in mapping PM2. 5 based on satellite retrievals and ground observations[J]. Geosci Front, 2024, 15(1): 101686. DOI: 10.1016/j.gsf.2023.101686. [15] Fu JB, Tang D, Grieneisen ML, et al. A machine learning-based approach for fusing measurements from standard sites, low-cost sensors, and satellite retrievals: Application to NO2 pollution hotspot identification[J]. Atmos Environ, 2023, 302: 119756: 119756. DOI: 10.1016/j.atmosenv.2023.119756. [16] Huete AR, Didan K, Leeuwen WJ DV, et al. MODIS VEGETATION INDEX (MOD 13) ALGORITHM THEORETICAL BASIS DOCUMENT Version 3. 1 Principal Investigators, F, 1999[C]. [17] Mills IC, Atkinson RW, Kang S, et al. Quantitative systematic review of the associations between short-term exposure to nitrogen dioxide and mortality and hospital admissions[J]. BMJ Open, 2015, 5(5): e006946. DOI: 10.1136/bmjopen-2014-006946. [18] Mills NL, Törnqvist H, Robinson SD, et al. Diesel exhaust inhalation causes vascular dysfunction and impaired endogenous fibrinolysis[J]. Circulation, 2005, 112(25): 3930-3936. DOI: 10.1161/CIRCULATIONAHA.105.588962. [19] Pekkanen J, Brunner EJ, Anderson HR, et al. Daily concentrations of air pollution and plasma fibrinogen in London[J]. Occup Environ Med, 2000, 57(12): 818-822. DOI: 10.1136/oem.57.12.818. [20] Veras MM, Damaceno-Rodrigues NR, Caldini EG, et al. Particulate urban air pollution affects the functional morphology of mouse placenta[J]. Biol Reprod, 2008, 79(3): 578-584. DOI: 10.1095/biolreprod.108.069591. [21] van den Hooven EH, Pierik FH, de Kluizenaar Y, et al. Air pollution exposure and markers of placental growth and function: the generation R study[J]. Environ Health Perspect, 2012, 120(12): 1753-1759. DOI: 10.1289/ehp.1204918. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 70
- HTML全文浏览量: 23
- PDF下载量: 15
- 被引次数: 0