

Systematic review of the incidence and risk factors of hypertension among HIV-positive individuals
-
摘要:
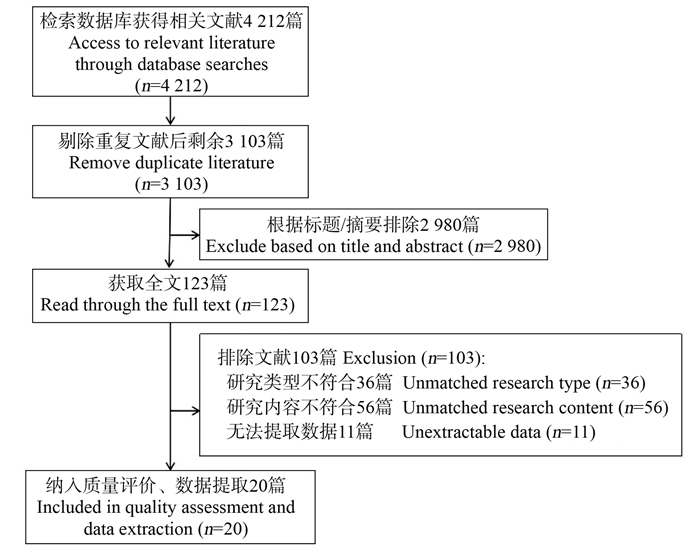
目的 对人类免疫缺陷病毒(human immunodeficiency virus, HIV)阳性者高血压的发病密度和影响因素进行系统综述,旨在探索HIV阳性者发生高血压的影响因素及潜在的机制。 方法 通过中国知网、万方数据知识服务平台、PubMed、EMbase、Web of Science和Medline数据库系统检索HIV阳性者中高血压发病的相关文献,摘录基本信息、发病密度及影响因素。 结果 最终纳入20篇研究,研究包含北美洲国家5篇,非洲国家5篇,亚洲国家4篇,欧洲国家2篇,多中心研究4篇。HIV阳性者的高血压发病密度为26.0/1 000人年~320.1/1 000人年。HIV阳性者新发高血压的影响因素包括传统因素如年龄、性别、种族、BMI和腹部肥胖、糖尿病、肾病和血脂异常; 特异性的影响因素包括HIV感染时间、抗病毒治疗(antiretroviral therapy, ART)时长和ART药物等。 结论 HIV阳性者的高血压发病密度较高,且地理差异较大。HIV阳性者新发高血压的传统影响因素作用比较确定,需要在HIV阳性者的生活方式中实施初级预防的策略和措施。然而,HIV和ART相关的影响因素对高血压发生的作用尚不清楚,需要进行前瞻性研究来确定HIV特异性因素的影响,以更好地了解HIV阳性者的高血压流行病学。 -
关键词:
- 人类免疫缺陷病毒阳性 /
- 高血压 /
- 发病密度
Abstract:Objective To systematically review the incidence density and influencing factors of hypertension in HIV positive people in order to explore the potential mechanisms of hypertension in HIV positive individuals. Methods We search literature related to incident hypertension among HIV-positive individuals through CNKI, Wanfang, PubMed, EMbase, Web of Science and Medline, databases and the basic information, incidence density and risk factors were extracted. Results A total of 20 studies were included, comprising 5 from North America, 5 from Africa, 4 from Asia, 2 from Europe, and 4 from multicenter studies. The incidence density of hypertension in HIV-positive individuals ranged from 26.0 to 320.1 per 1 000 person-years. The risk factors of incident hypertension in HIV-positive individuals include traditional risk factors such as age, gender, race, BMI and abdominal obesity, diabetes, kidney disease, dyslipidemia, etc. HIV-specific factors included time of HIV infection, duration of antiviral therapy (ART), and antiviral drugs. Conclusions The incidence density of hypertension is relatively high among HIV-positive individuals, and the geographical variations are particularly pronounced. The contribution of traditional risk factors to incident hypertension among HIV-positive individuals is well established, underscoring the importance of implementing comprehensive strategies and interventions for primary prevention within this population's lifetstyles. However, the role of HIV and ART-related risk factors in hypertension remains unclear, and prospective studies are needed to better elucidate the epidemiology of hypertension in HIV-positive individuals. -
Key words:
- Human immunodeficiency virus positive /
- Hypertension /
- Incidence density
-
表 1 HIV阳性者高血压发病密度及影响因素
Table 1. Incidence density and risk factors of hypertension among HIV/AIDS individuals
地区
District发表时间
Year研究类型
Type新发高血压诊断标准
Diagnostic criteria随访时间
Follow-up time研究地点
Research site北美洲
North America2013[11] 队列研究
Cohort study基线血压正常,随访2次测量≥140/90 mmHg或有高血压诊断史或诊断史且服用降压药
Baseline blood pressure within normal range, with follow-up measurements ≥140/90 mmHg or a history of hypertension diagnosis or a diagnosis history and taking antihypertensive medication2001—2006 美国
United States2013[21] 队列研究
Cohort study基线血压正常,随访接受任何高血压治疗
Baseline blood pressure within normal range, with follow-up receiving any hypertension treatment1998—2011 美国
United States2016[13] 队列研究
Cohort study基线血压正常,随访高血压诊断史
Baseline blood pressure within normal range, with follow-up history of hypertension diagnosis1996—2013 美国
United States2018[29] 队列研究
Cohort study基线血压正常,随访2次测量≥140/90 mmHg或服用降压药
Baseline blood pressure within normal range, with follow-up measurements ≥140/90 mmHg on two occasions or taking antihypertensive medication2005—2009 海地
Haiti2022[40] 队列研究
Cohort study基线血压正常,随访3次测量≥140/90 mmHg或有高血压诊断史
Baseline blood pressure within normal range, with follow-up measurements ≥140/90 mmHg on three occasions or a history of hypertension diagnosis2014—2019 美国
United States非洲Africa 2020[10] 前瞻性研究Prospective study 基线血压正常,随访2次测量≥140/90 mmHg
Baseline blood pressure within normal range, with follow-up measurements ≥140/90 mmHg1年Year 加纳
Ghana2015[14] 纵向研究Longitudinal study 基线血压正常,随访2次测量≥140/90 mmHg或服用降压药
Baseline blood pressure within normal range, with follow-up measurements ≥140/90 mmHg on two occasions or taking antihypertensive medication2010—2013 乌干达
Uganda2016[36] 队列研究
Cohort study基线血压正常,随访3次测量≥140/90 mmHg或服用降压药
Baseline blood pressure within normal range, with follow-up measurements ≥140/90 mmHg on three occasions or taking antihypertensive medication2005—2015 乌干达
Uganda2017[18] 纵向研究Longitudinal study 基线血压正常,随访2次测量≥140/90 mmHg
Baseline blood pressure within normal range, with follow-up measurements ≥140/90 mmHg on two occasions2013—2015 撒哈拉
Sahara2018[28] 队列研究
Cohort study基线血压正常,随访3次测量≥140/90 mmHg或一次测量≥180/110 mmHg或ART 3个月后有高血压诊断史或服用降压药
Baseline blood pressure within normal range, with follow-up measurements ≥140/90 mmHg on three occasions, or a single measurement ≥180/110 mmHg, or a history of hypertension diagnosis after 3 months of antiviral treatment, or taking antihypertensive medication2004—2016 南非
South Africa欧洲Europe 2012[23] 队列研究
Cohort study基线血压正常,随访2次测量≥140/90 mmHg或服用降压药
Baseline blood pressure within normal range, with follow-up measurements ≥140/90 mmHg on two occasions or taking antihypertensive medication2007—2010 挪威
Norway2017[16] 队列研究
Cohort study基线血压正常,随访2次测量≥140/90 mmHg或服用降压药
Baseline blood pressure within normal range, with follow-up measurements ≥140/90 mmHg on two occasions or taking antihypertensive medication2010—2017 意大利
Italy亚洲Asia 2021[37] 前瞻性研究Prospective study 基线血压正常,随访2次测量≥130/80 mmHg
Baseline blood pressure within normal range, with follow-up measurements ≥130/80 mmHg on two occasions2019—2020 埃塞俄比亚
Ethiopia2020[20] 队列研究
Cohort study基线血压正常,随访≥140/90 mmHg或高血压诊断史
Baseline blood pressure within normal range, with follow-up measurements ≥140/90 mmHg or a history of hypertension diagnosis2017—2019 中国
China2018[38] 队列研究
Cohort study基线血压正常,随访≥140/90 mmHg或服用降压药
Baseline blood pressure within normal range, with follow-up measurements ≥140/90 mmHg or taking antihypertensive medication2008—2016 韩国
Korea2020[39] 纵向研究Longitudinal study 基线血压正常,随访≥140/90 mmHg或服用降压药
Baseline blood pressure is normal, with follow-up measurements ≥140/90 mmHg or taking antihypertensive medication2008—2015 中国
China多中心
Multicenter2005[25] 队列研究
Cohort study基线血压正常,随访≥140/90 mmHg或服用降压药
Baseline blood pressure is normal, with follow-up measurements ≥140/90 mmHg or taking antihypertensive medication1999—2003 多中心
Multicenter2017[9] 队列研究
Cohort study基线血压正常,随访高血压诊断史并服用降压药
Baseline blood pressure within normal range, with follow-up history of hypertension diagnosis and taking antihypertensive medication2000—2013 多中心
Multicenter2018[26] 队列研究
Cohort study基线血压正常,随访≥140/90 mmHg或服用降压药
Baseline blood pressure is normal, with follow-up measurements ≥140/90 mmHg or taking antihypertensive medication1999—2013 多中心
Multicenter2022[41] 回顾性队列
Retrospective cohort study基线血压正常,随访2次测量≥140/90 mmHg或服用降压药
Baseline blood pressure is normal, with follow-up measurements ≥140/90 mmHg on two occasions or taking antihypertensive medication2012—2019 多中心
Multicenter地区
District年龄/岁
Age/years男性占比/%
Proportion of male/%样本量
Sample size治疗率
ART/%发病密度/1 000人年
Incidence density/1 000 person-years影响因素
Influenceing factorsNOS评分
NOS scoreHIV阳性
HIV+HIV阴性
HIV-HIV阳性
HIV+HIV阴性
HIV-北美洲
North America— 49.9 384 275 73.0 未治疗/治疗
女性:160.0/90.0
男性:220.0/170.0
Untreated/treated
Female: 160.0/90.0
Male: 220.0/170.0女性:140.0男性:170.0
Female: 140.0 Male: 170.06 43.0 80.0 2 390 84.0 64.1 年龄增加↑、黑人种族↑、体重升高↑、糖尿病↑
Age increase↑, Black ethnicity↑, weight gain↑, diabetes↑5 35.0 72.0 3 141 90.0 34.4 年龄增加↑、BMI≥30 kg/m2↑、糖尿病↑、最大肌酐≥1.4 mg/dL↑、可卡因↑、烟草↓、西班牙裔美国人↓
Age increase↑, BMI ≥ 30 kg/m2↑, diabetes↑, maximum creatinine≥ 1.4 mg/dL ↑, cocaine use↑, tobacco use↓, Hispanic Americans↓6 39.0 42.0 816 100.0 34.1 年龄增加↑、BMI高↑、IL-6升高↑
Age increase↑, high BMI↑, elevated IL-6↑6 47.0 71.5 2 274 — 63.0 4 非洲Africa — 25.0 443 100.0 320.1 年龄增加↓、病载量对数↑、泰诺福韦↑
Age decrease↓, logarithm of viral load increase↑, Tenofovir↑5 32.0 33.0 3 389 100.0 111.5 年龄增加↑、男性↑、BMI≥30 kg/m2↑、最小CD4+ T细胞计数<100个/μL↑
Age increase↑, male↑, BMI ≥ 30 kg/m2↑, minimum CD4+ T cell count<100 cells/μL↑6 34.0 30.0 230 100.0 31.7 年龄增加↑、男性↑、BMI≥25 kg/m2↑、最小CD4+ T细胞计数<100个/μL↑、ART后6个月D-二聚体水平↓
Age increase ↑, male ↑, BMI ≥25 kg/m2↑, minimum CD4 + T cell count<100 cells/μL↑, decreased D-dimer levels after 6 months of ART↓6 38.2 38.4 834 75.5 120.0 年龄增加↑、BMI高↑、eGFR<60 /ml(min·1.73 m2)↑
Age increase↑, high BMI↑, eGFR<60 /ml(min·1.73 m2)↑6 37.0 60.8 60 570 100.0 54.4 年龄增加↑、男性↑、BMI增加↑、基线正常高值血压↑、CD4+ T细胞计数<50个/μL↑、奈韦拉平↑、齐多夫定↑、司他夫定↑
Age increase↑, male↑, BMI increase↑, baseline hypertension with high values↑, CD4+ T cell count<50 cells/μL↑, Nelfinavir ↑, Zidovudine↑, Sustiva↑4 欧洲Europe 43.0 72.1 434 75.8 29.8 HIV感染时间↑、ART时长↑、尿白蛋白排泄异常↑
Increased duration of HIV infection↑, prolonged ART duration↑, increased abnormal urinary albumin excretion↑5 46.4 70.9 961 93.9 50.1 年龄增加↑、BMI增加↑、估算的心血管风险↑、基线血压高↑、HIV临床分期重↑
Age increase↑, BMI increase↑, elevated estimated cardiovascular risk↑, high baseline blood pressure↑, advanced HIV clinical stage increase↑5 亚洲Asia 35.0 48.7 302 100.0 196.2 男性↑, 年龄增加↑, BMI较高↑, 糖尿病↑, AZT用药史↑
Increased male gender↑, age increase↑, higher BMI↑, elevated diabetes↑, history of AZT medication use↑4 52.7 76.9 229 — 90.3 普通型肥胖↑、腹部肥胖↑
Increased general obesity↑, abdominal obesity↑5 — 92.7 6 493 100.0 40.0 年龄增加↑、男性↑、ART依从性低↑、预防性抗生素(阿巴卡韦)↑
Age increase↑, male gender increase↑, low ART adherence↑, increased use of prophylactic antibiotic (Abacavir)↑5 35.2 75.2 984 100.0 76.0 BMI高↑、基线CD4+ T细胞计数高↑、最近病毒载量增加↑; 齐多夫定/泰诺福韦(相比司他夫定)↓, 最近CD4+/CD8+比值↓
High BMI↑, high baseline CD4+ T cell count↑, recent viral load increase↑; Zidovudine/Tenofovir (compared to Sustiva) decrease↓; recent CD4+/CD8+ ratio decrease↓6 多中心
Multicenter— 72.6 8 984 — 72.1 年龄增加↑、男性↑、BMI高↑、基线血压高↑、总胆固醇高↑、临床脂肪代谢障碍↑
Age increase↑, male↑, high BMI↑, high baseline blood pressure↑, high total cholesterol↑, increased clinical lipid metabolism disorders↑6 — — 68 405 — 26.0 黑人种族↑ Black ethnicity↑ 5 38.0 72.2 33 278 68.4 34.2 年龄增加↑、男性↑、黑人种族↑、BMI高↑、糖尿病↑、血脂异常↑、eGFR低↑、CD4+ T细胞计数低↑、奈韦拉平↑
Indinavir/ritonavir↑ Age increase↑, male↑, Black ethnicity increase↑, high BMI↑, elevated diabetes↑, abnormal blood lipid levels↑, decreased eGFR↑, low CD4+ T cell count↑, increased use of Nelfinavir↑, increased use of Indinavir/Ritonavir↑4 43.0 73.4 4 606 54.0 126.2 基于INSTI/PI的治疗方案↑、基线CD4+ T细胞计数<350个/μL↑、基线未治疗↑、BMI≥30 kg/m2↑
Tment regimen based on INSTI/PI↑, baseline CD4+ T cell count<350 cells/μL↑, treatment-naive at baseline↑, BMI ≥ 30 kg/m2↑5 注:1. ↑与新发高血压呈统计学正相关;↓与新发高血压呈统计学负相关。
2. ART,抗病毒治疗;NOS, 纽卡斯尔—渥太华量表;eGFR,肾小球滤过率估算值;AZT,齐多夫定;Indinavir/Ritonavir,茚地那韦/利托那韦;INSTI/PI, 整合酶链转移抑制剂/蛋白酶抑制剂。
3. “—”表示未提取到相关数。
Note: 1. ↑ indicates a positive correlation with incident hypertension; ↓ indicates a negative correlation with incident hypertension.
2. ART, antiretroviral therapy; NOS, Newcastle-Ottawa scale; eGFR,estimated glomerular filtration rate;AZT, zidovudine; Indinavir/ritonavir, Indinavir/ritonavir; INSTI/PI, integrase strand transfer inhibitor/protease inhibitor.
3. "—" indicates that no relevant data has been extracted. 下载: 导出CSV
下载: 导出CSV
-
[1] Nat Cheza A, Tlou B, Zhou DT. Incidence of non-communicable diseases (NCDs) in HIV patients on ART in a developing country: case of Zimbabwe's Chitungwiza Central Hospital-a retrospective cohort study (2010-2019)[J]. PLoS One, 2021, 16(5): e0252180. DOI: 10.1371/journal.pone.0252180. [2] Smith CJ, Ryom L, Weber R, et al. Trends in underlying causes of death in people with HIV from 1999 to 2011 (D: a: d): a multicohort collaboration[J]. Lancet, 2014, 384(9939): 241-248. DOI: 10.1016/S0140-6736(14)60604-8. [3] Smit M, Brinkman K, Geerlings S, et al. Future challenges for clinical care of an ageing population infected with HIV: a modelling study[J]. Lancet Infect Dis, 2015, 15(7): 810-818. DOI: 10.1016/S1473-3099(15)00056-0. [4] Chiwandire N, Zungu N, Mabaso M, et al. Trends, prevalence and factors associated with hypertension and diabetes among South African adults living with HIV, 2005-2017[J]. BMC Public Health, 2021, 21(1): 462. DOI: 10.1186/s12889-021-10502-8. [5] 徐小慧, 何春燕, 何纳, 等. HIV感染者高血压患病率及其影响因素研究近况[J]. 上海预防医学, 2021, 33(12): 1166-1175. DOI: 10.19428/j.cnki.sjpm.2021.20765.Xu XH, He CY, He N, et al. A systematic review of the prevalence and influence factors of hypertension among HIV-infected individuals[J]. Shanghai J Prev Med, 2021, 33(12): 1166-1175. DOI: 10.19428/j.cnki.sjpm.2021.20765. [6] Sarfo FS, Norman B, Appiah L, et al. Factors associated with incidence of stroke and heart failure among people living with HIV in Ghana: evaluating vascular event risk while on long-term antiretroviral suppressive therapy (EVERLAST) study[J]. J Clin Hypertens, 2021, 23(6): 1252-1259. DOI: 10.1111/jch.14255. [7] Muiru AN, Madden E, Chilingirian A, et al. The incidence of and risk factors for hospitalized acute kidney injury among people living with HIV on antiretroviral treatment[J]. HIV Med, 2022, 23(6): 611-619. DOI: 10.1111/hiv.13216. [8] Guzman VA, Cham H, Gutierrez J, et al. The longitudinal effects of blood pressure and hypertension on neurocognitive performance in people living with HIV[J]. J Acquir Immune Defic Syndr, 2021, 88(2): 197-205. DOI: 10.1097/QAI.0000000000002740. [9] Wong C, Gange SJ, Buchacz K, et al. First occurrence of diabetes, chronic kidney disease, and hypertension among North American HIV-infected adults, 2000-2013[J]. Clin Infect Dis, 2017, 64(4): 459-467. DOI: 10.1093/cid/ciw804. [10] Sarfo FS, Singh A, Tagge R, et al. Duration of antiretroviral therapy among people living with HIV and incidence of hypertension in Ghana[J]. J Clin Hypertens, 2020, 22(12): 2361-2371. DOI: 10.1111/jch.14088. [11] Factor SH, Lo Y, Schoenbaum E, et al. Incident hypertension in older women and men with or at risk for HIV infection[J]. HIV Med, 2013, 14(6): 337-346. DOI: 10.1111/hiv.12010. [12] Tripathi A, Jerrell JM, Skelton TN, et al. Incidence of primary hypertension in a population-based cohort of HIV-infected compared with non-HIV-infected persons and the effect of combined antiretroviral therapy[J]. J Am Soc Hypertens, 2015, 9(5): 351-357. DOI: 10.1016/j.jash.2015.01.007. [13] Okeke NL, Davy T, Eron JJ, et al. Hypertension among HIV-infected patients in clinical care, 1996-2013[J]. Clin Infect Dis, 2016, 63(2): 242-248. DOI: 10.1093/cid/ciw223. [14] Okello S, Kanyesigye M, Muyindike WR, et al. Incidence and predictors of hypertension in adults with HIV-initiating antiretroviral therapy in south-western Uganda[J]. J Hypertens, 2015, 33(10): 2039-2045. DOI: 10.1097/HJH.0000000000000657. [15] Lucas GM, Lau B, Atta MG, et al. Chronic kidney disease incidence, and progression to end-stage renal disease, in HIV-infected individuals: a tale of two races[J]. J Infect Dis, 2008, 197: 1548-1557. DOI: 10.1086/587994. [16] De Socio GV, Ricci E, Maggi P, et al. Time trend in hypertension prevalence, awareness, treatment, and control in a contemporary cohort of HIV-infected patients: the HIV and hypertension study[J]. J Hypertens, 2017, 35(2): 409-416. DOI: 10.1097/HJH.0000000000001150. [17] Dyer AR, Liu K, Walsh M, et al. Ten-year incidence of elevated blood pressure and its predictors: the CARDIA study. Coronary artery risk development in (young) adults[J]. J Hum Hypertens, 1999, 13(1): 13-21. DOI: 10.1038/sj.jhh.1000740. [18] Rodríguez-Arbolí E, Mwamelo K, Kalinjuma AV, et al. Incidence and risk factors for hypertension among HIV patients in rural Tanzania-A prospective cohort study[J]. PLoS One, 2017, 12(3): e0172089. DOI: 10.1371/journal.pone.0172089. [19] Freitas P, Carvalho D, Santos AC, et al. Central/peripheral fat mass ratio is associated with increased risk of hypertension in HIV-infected patients[J]. J Clin Hypertens, 2012, 14(9): 593-600. DOI: 10.1111/j.1751-7176.2012.00671.x. [20] Xu XH, Chen XX, Lin HJ, et al. General and abdominal obesity and incident hypertension among people living with HIV on antiretroviral therapy[J]. AIDS Care, 2021, 33(12): 1616-1620. DOI: 10.1080/09540121.2020.1852158. [21] Krauskopf K, Van Natta ML, Danis RP, et al. Correlates of hypertension in patients with AIDS in the era of highly active antiretroviral therapy[J]. J Int Assoc Provid AIDS Care, 2013, 12(5): 325-333. DOI: 10.1177/2325957413491432. [22] Ferrannini E, Cushman WC. Diabetes and hypertension: the bad companions[J]. Lancet, 2012, 380(9841): 601-610. DOI: 10.1016/S0140-6736(12)60987-8. [23] Manner IW, Baekken M, Oektedalen O, et al. Hypertension and antihypertensive treatment in HIV-infected individuals. A longitudinal cohort study[J]. Blood Press, 2012, 21(5): 311-319. DOI: 10.3109/08037051.2012.680742. [24] Cowley AW Jr, Roman RJ. The role of the kidney in hypertension[J]. JAMA, 1996, 275(20): 1581-1589. [25] Thiébaut R, El-Sadr WM, Friis-Møller N, et al. Predictors of hypertension and changes of blood pressure in HIV-infected patients[J]. Antivir Ther, 2005, 10(7): 811-823. DOI: 10.1177/135965350501000706. [26] Hatleberg CI, Ryom L, Monforte AD, et al. Association between exposure to antiretroviral drugs and the incidence of hypertension in HIV-positive persons: the data collection on adverse events of anti-HIV drugs (D: a: d) study[J]. HIV Med, 2018, 19(9): 605-618. DOI: 10.1111/hiv.12639. [27] Srikanth S, Deedwania P. Management of dyslipidemia in patients with hypertension, diabetes, and metabolic syndrome[J]. Curr Hypertens Rep, 2016, 18(10): 76. DOI: 10.1007/s11906-016-0683-0. [28] Brennan AT, Jamieson L, Crowther NJ, et al. Prevalence, incidence, predictors, treatment, and control of hypertension among HIV-positive adults on antiretroviral treatment in public sector treatment programs in South Africa[J]. PloS one, 2018, 13(10): e0204020. DOI: 10.1371/journal.pone.0204020. [29] Batavia AS, Severe P, Lee MH, et al. Blood pressure and mortality in a prospective cohort of HIV-infected adults in Port-au-Prince, Haiti[J]. J Hypertens, 2018, 36(7): 1533-1539. DOI: 10.1097/HJH.0000000000001723. [30] Harrison DG, Guzik TJ, Lob HE, et al. Inflammation, immunity, and hypertension[J]. Hypertension, 2011, 57(2): 132-140. DOI: 10.1161/HYPERTENSIONAHA.110.163576. [31] Cattelan AM, Trevenzoli M, Sasset L, et al. Indinavir and systemic hypertension[J]. AIDS, 2001, 15(6): 805-807. DOI: 10.1097/00002030-200104130-00021. [32] Seaberg EC, Muñoz A, Lu M, et al. Association between highly active antiretroviral therapy and hypertension in a large cohort of men followed from 1984 to 2003[J]. AIDS, 2005, 19(9): 953-960. DOI: 10.1097/01.aids.0000171410.76607.f8. [33] Crane HM, Van Rompaey SE, Kitahata MM. Antiretroviral medications associated with elevated blood pressure among patients receiving highly active antiretroviral therapy[J]. AIDS, 2006, 20(7): 1019-1026. DOI: 10.1097/01.aids.0000222074.45372.00. [34] Palacios R, Santos J, García A, et al. Impact of highly active antiretroviral therapy on blood pressure in HIV-infected patients. A prospective study in a cohort of naive patients[J]. HIV Med, 2006, 7(1): 10-15. DOI: 10.1111/j.1468-1293.2005.00333.x. [35] Xu YN, Chen XG, Wang K. Global prevalence of hypertension among people living with HIV: a systematic review and meta-analysis[J]. J Am Soc Hypertens, 2017, 11(8): 530-540. DOI: 10.1016/j.jash.2017.06.004. [36] Okello S, Asiimwe SB, Kanyesigye M, et al. D-dimer levels and traditional risk factors are associated with incident hypertension among HIV-infected individuals initiating antiretroviral therapy in Uganda[J]. J Acquir Immune Defic Syndr, 2016, 73(4): 396-402. DOI: 10.1097/QAI.0000000000001074. [37] Mulugeta H, Afenigus AD, Haile D, et al. Incidence and predictors of hypertension among HIV patients receiving ART at public health facilities, Northwest Ethiopia: a one-year multicenter prospective follow-up study[J]. HIV/AIDS, 2021, 13: 889-901. DOI: 10.2147/HIV.S329838. [38] Kim J, Bang JH, Shin JY, et al. Hypertension risk with abacavir use among HIV-infected individuals: a nationwide cohort study[J]. Yonsei Med J, 2018, 59(10): 1245-1252. DOI: 10.3349/ymj.2018.59.10.1245. [39] Fan HW, Guo FP, Hsieh E, et al. Incidence of hypertension among persons living with HIV in China: a multicenter cohort study[J]. BMC Public Health, 2020, 20(1): 834. DOI: 10.1186/s12889-020-08586-9. [40] Remch M, Franceschini N, Davy-Mendez T, et al. Hypertension burden, treatment, and control among people with HIV at a clinical care center in the Southeastern US, 2014-2019[J]. AIDS Care, 2023, 35(10): 1594-1603. DOI: 10.1080/09540121.2022.2148626. [41] Byonanebye DM, Polizzotto MN, Neesgaard B, et al. Incidence of hypertension in people with HIV who are treated with integrase inhibitors versus other antiretroviral regimens in the RESPOND cohort consortium[J]. HIV Med, 2022, 23(8): 895-910. DOI: 10.1111/hiv.13273. -

 点击查看大图
点击查看大图
图(1) / 表(1)
计量
- 文章访问数: 125
- HTML全文浏览量: 31
- PDF下载量: 20
- 被引次数: 0