

Joinpoint regression and age-period-cohort analysis of mortality trends of cardiovascular disease attributable to kidney dysfunction in China
-
摘要:
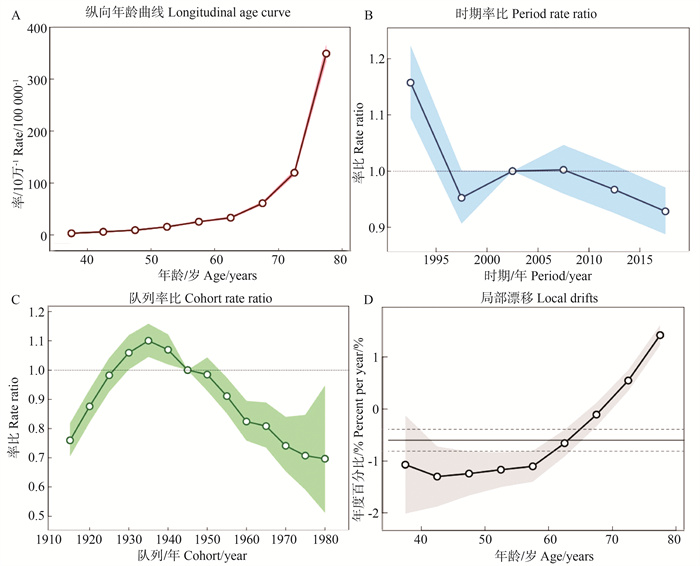
目的 分析1990-2019年我国肾功能损伤所致心血管病(cardiovascular disease attributed to kidney dysfunction, KI-CVD)死亡率变化趋势,并评估年龄、时期及队列对KI-CVD死亡率的影响。 方法 利用2019全球疾病负担研究(global burden of disease study 2019, GBD 2019)中1990-2019年中国KI-CVD死亡资料,通过Joinpoint回归模型分析粗死亡率(crude death rate, CDR)及年龄标化死亡率(age-standardized death rate, ASDR)的年度变化百分比(annual percent change, APC)和平均年度变化百分比(average annual percent change, AAPC); 建立年龄-时期-队列模型分析年龄、时期及队列对KI-CVD的影响。 结果 归因于KI-CVD的CDR总体呈上升趋势,从1990年的12.65/10万上升至2019年的26.49/10万,年均上升3.35%(AAPC=3.35%, 95% CI: 3.06%~3.64%),ASDR总体呈上升趋势(AAPC=0.70%, 95% CI: 0.39%~1.00%)。APC模型显示:1990-2019年归因于KI-CVD的死亡率随年龄增长呈上升趋势,随时间推移呈先下降后上升至平稳再下降的趋势,以2000-2004年为参考,1990-1994年死亡风险相对较高,2015-2019年死亡相对风险较低。队列效应显示呈倒“U”型,1911-1939年队列死亡率呈上升趋势,1931-1939年死亡风险达到高峰(RR=1.100, 95% CI: 1.046~1.158)后呈下降趋势。 结论 1990-2019年我国归因于KI-CVD的CDR总体呈上升趋势,死亡风险受年龄、时期及队列效应的影响。 -
关键词:
- 肾功能损伤 /
- 心血管病 /
- 死亡率 /
- Joinpoint回归模型 /
- 年龄-时期-队列模型
Abstract:Objective To analyze the long-term trends and effects of age, period and cohort on cardiovascular disease mortality attributed to kidney dysfunction (KI-CVD) in China from 1990 to 2019. Methods Data on the absolute number, crude death rate (CDR) and age-standardized mortality (ASDR) for KI-CVD in China were collected from global burden of disease study 2019. The annual percentage change (APC) and average annual percentage change (AAPC) were calculated to analyze the trends of CDR and ASDR by Joinpoint regression model. The age, period and cohort effects were estimated using an age-period-cohort model. Results The CDR of KI-CVD was generally increasing, from 12.65 per 100 000 in 1990 to 26.49 per 100 000 in 2019 (AAPC=3.35%, 95% CI: 3.06%-3.64%). ASDR showed a slight increase (AAPC=0.70%, 95% CI: 0.39%-1.00%). APC model analysis showed that from 1990 to 2019, age effect exhibited an upward trend with the increase of age. Period effect decreased first, then increased to steady and then decreased over time. Taking 2000-2004 as the reference group, the rate ratio of death was higher in 1990-1994, and lower in 2015-2019. Cohort effect showed an inverted "U" shape, with an upward trend in 1911-1939 cohort, peaking in 1931-1939 (RR=1.100, 95% CI: 1.046-1.158), then decreasing with the year of birth. Conclusions The CDR of KI-CVD in China is generally on the rise from 1990 to 2019 and the risk of death is affected by age, period and cohort effect. -

图 1 1990-2019年我国KI-CVD的CDR和ASDR长期变化趋势
CDR:粗死亡率;ASDR:年龄标化死亡率。
Figure 1. Long-term trends for CDR and ASDR of KI-CVD in China, 1990-2019
CDR: crude death rate; ASDR: age-standardized death rates.

图 2 1990-2019年我国KI-CVD死亡率APC变化趋势
A:年龄效应;B:时期效应;C:队列效应;D:局部漂移。
Figure 2. Age-period-cohort effect for CDR of KI-CVD in China, 1990-2019
A: age effects; B: period effects; C: cohort effects; D: local drift.
表 1 1990年和2019年中国KI-CVD死亡病例数、CDR及ASDR
Table 1. Absolute number, crude death rate and ASDR for KI-CVD in 1990 and 2019 in China
年份
Year变量
Variable全人群(95% UI)
Both(95% UI)男性(95% UI)
Male(95% UI)女性(95% UI)
Female(95% UI)1990 死亡例数/万Death number/10 000 14.97(11.91~18.48) 7.29(5.73~9.29) 7.68(5.89~9.91) CDR/10万-1 CDR/100 000-1 12.65(10.06~15.60) 11.95(9.38~15.21) 13.40(10.27~17.28) ASDR/10万-1 ASDR/100 000-1 22.79(17.55~28.80) 24.90(19.13~31.54) 21.51(16.12~27.91) 2019 死亡例数/万Death number/10 000 37.68(28.54~48.01) 19.43(14.41~25.55) 18.25(13.08~24.57) CDR/10万-1 CDR/100 000-1 26.49(20.06~33.75) 26.81(19.88~35.25) 26.16(18.75~35.22) ASDR/10万-1 ASDR/100 000-1 22.59(16.91~29.26) 27.32(19.87~36.15) 19.48(13.81~26.34) 注:UI,不确定区间;CDR,粗死亡率;ASDR,年龄标化死亡率。
Note: UI, uncertainty interval; CDR, crude death rate; ASDR, age-standardized death rates. 下载: 导出CSV
下载: 导出CSV
表 2 1990-2019年中国不同性别KI-CVD的CDR和ASDR趋势变化
Table 2. Long trends for CDR and ASDR of KI-CVD by gender in China, 1990-2019
变量
VariableCDR/100 000-1 年份
YearAPC/%
(95% CI)t(P)值
valueAAPC/%
(95% CI)Z(P)值value 全人群Both 1990-1998 0.16(-0.11~0.43) 1.30(0.210) 3.35(3.06~3.64) 23.77(<0.001) 1998-2004 7.34(6.75~7.93) 24.31(<0.001) 2004-2007 1.64(-0.84~ 4.19) -4.65(<0.001) 2007-2010 3.99(1.45~6.59) 1.41(0.180) 2010-2017 2.34(1.92~2.77) -1.37(0.190) 2017-2019 -0.61(-3.03~1.88) -2.52(0.020) 男性Male 1990-1995 0.21(-0.71~1.14) 0.49(0.630) 3.65(3.37~3.94) 26.64(<0.001) 1995-1999 2.49(0.39~4.63) 2.14(0.050) 1999-2004 7.25(5.86~8.67) 4.01(0.001) 2004-2012 3.40(2.83~3.98) -5.56(<0.001) 2012-2017 2.43(1.10~3.78) -1.43(0.175) 2017-2019 -1.63(-5.62~2.53) -2.01(0.060) 女性Female 1990-1996 -0.71(-1.31~-0.10) -2.50(0.030) 3.04(2.73~3.35) 20.55(<0.001) 1996-1999 1.95(-1.67~5.71) 1.55(0.140) 1999-2004 7.93(6.71~9.18) 3.25(0.010) 2004-2007 1.24(-2.35~4.97) -3.64(0.020) 2007-2017 2.40(2.06~2.74) 0.67(0.510) 2017-2019 0.27(-3.30~3.96) -1.25(0.230) 全人群Both 1990-1998 -1.55(-1.76~-1.33) -15.43(<0.001) 0.70(0.39~1.00) 4.71(<0.001) 1998-2004 4.57(4.10~5.04) 21.61(<0.001) 2004-2007 -0.88(-2.84~1.12) -0.96(0.350) 2007-2010 1.42(-0.59~3.46) 1.51(0.150) 2010-2017 -1.10(-1.44~-0.77) -7.09(<0.001) 2017-2019 -3.84(-5.74~-1.90) -4.23(<0.001) 男性Male 1990-1998 -0.91(-1.13~-0.69) -8.91(<0.001) 1.13(0.83~1.43) 7.68(<0.001) 1998-2004 4.36(3.89~4.84) 20.28(<0.001) 2004-2007 0.07(-1.95~2.12) 0.07(0.940) 2007-2011 2.21(1.18~3.25) 4.64(<0.001) 2011-2017 -1.16(-1.61~-0.71) -5.55(<0.001) 2017-2019 -4.85(-6.77~-2.89) -5.28(<0.001) 女性Female 1990-1998 -2.10(-2.47~-1.73) -12.17(<0.001) 0.35(0.02~0.67) 2.20(0.040) 1998-2004 4.58(3.78~ 5.40) 12.52(<0.001) 2004-2011 -0.48(-1.06~0.10) -1.77(0.090) 2011-2014 -2.21(-5.53~1.23) -1.39(0.190) 2014-2017 -0.29(-3.68~3.21) -0.18(0.860) 2017-2019 -3.92(-7.19~-0.54) -2.50(0.030) 注:CDR,粗死亡率;APC,年度变化百分比;AAPC,平均年度变化百分比;ASDR,年龄标化死亡率。
Notes: CDR, crude death rate; APC, annual percent change; AAPC, average annual percent change; ASDR, age-standardized death rates.
下载: 导出CSV
-
[1] Mensah GA, Fuster V, Murray CJL, et al. Global burden of cardiovascular diseases and risks, 1990-2022[J]. J Am Coll Cardiol, 2023, 82(25): 2350-2473. DOI: 10.1016/j.jacc.2023.11.007. [2] 中国心血管健康与疾病报告编写组. 中国心血管健康与疾病报告2022概要[J]. 中国循环杂志, 2023, 38(6): 583-612. DOI: 10.3969/j.issn.1000-3614.2023.06.001.The Writing Committee of the Report on Cardiovascular Health and Diseases in China. Report on cardiovascular health and diseases in China 2022: an updated summary[J]. Chin Circul J, 2023, 38(6): 583-612. DOI: 10.3969/j.issn.1000-3614.2023.06.001. [3] Münzel T, Hahad O, Sørensen M, et al. Environmental risk factors and cardiovascular diseases: a comprehensive expert review[J]. Cardiovasc Res, 2022, 118(14): 2880-2902. DOI: 10.1093/cvr/cvab316. [4] Fuchs FD, Whelton PK. High blood pressure and cardiovascular disease[J]. Hypertension, 2020, 75(2): 285-292. DOI: 10.1161/HYPERTENSIONAHA.119.14240. [5] Han H, Wang Y, Li TT, et al. Sleep duration and risks of incident cardiovascular disease and mortality among people with type 2 diabetes[J]. Diabetes Care, 2023, 46(1): 101-110. DOI: 10.2337/dc22-1127. [6] Ortiz A, Wanner C, Gansevoort R, et al. Chronic kidney disease as cardiovascular risk factor in routine clinical practice: a position statement by the Council of the European Renal Association[J]. Eur J Prev Cardiol, 2022, 29(17): 2211-2215. DOI: 10.1093/eurjpc/zwac186. [7] Jager KJ, Kovesdy C, Langham R, et al. A single number for advocacy and communication-worldwide more than 850 million individuals have kidney diseases[J]. Nephrol Dial Transplant, 2019, 34(11): 1803-1805. DOI: 10.1093/ndt/gfz174. [8] GBD Chronic Kidney Disease Collaboration. Global, regional, and national burden of chronic kidney disease, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017[J]. Lancet, 2020, 395(10225): 709-733. DOI: 10.1016/S0140-6736(20)30045-3. [9] Wang H, Zhang H, Zou ZY. Changing profiles of cardiovascular disease and risk factors in China: a secondary analysis for the Global Burden of Disease Study 2019[J]. Chin Med J, 2023, 136(20): 2431-2441. DOI: 10.1097/cm9.0000000000002741. [10] GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019[J]. Lancet, 2020, 396(10258): 1204-1222. DOI: 10.1016/S0140-6736(20)30925-9. [11] Foreman KJ, Marquez N, Dolgert A, et al. Forecasting life expectancy, years of life lost, and all-cause and cause-specific mortality for 250 causes of death: reference and alternative scenarios for 2016-40 for 195 countries and territories[J]. Lancet, 2018, 392(10159): 2052-2090. DOI: 10.1016/S0140-6736(18)31694-5. [12] Lu JL, Mu YM, Su Q, et al. Reduced kidney function is associated with cardiometabolic risk factors, prevalent and predicted risk of cardiovascular disease in Chinese adults: results from the REACTION study[J]. J Am Heart Assoc, 2016, 5(7): e003328. DOI: 10.1161/JAHA.116.003328. [13] Guo YD, Cui LF, Ye PP, et al. Change of kidney function is associated with all-cause mortality and cardiovascular diseases: results from the Kailuan study[J]. J Am Heart Assoc, 2018, 7(21): e010596. DOI: 10.1161/JAHA.118.010596. [14] Vashistha V, Lee M, Wu YL, et al. Low glomerular filtration rate and risk of myocardial infarction: a systematic review and meta-analysis[J]. Int J Cardiol, 2016, 223: 401-409. DOI: 10.1016/j.ijcard.2016.07.175. [15] Connelly PJ, Azizi Z, Alipour P, et al. The importance of gender to understand sex differences in cardiovascular disease[J]. Can J Cardiol, 2021, 37(5): 699-710. DOI: 10.1016/j.cjca.2021.02.005. [16] Costantino S, Paneni F, Cosentino F. Ageing, metabolism and cardiovascular disease[J]. J Physiol, 2016, 594(8): 2061-2073. DOI: 10.1113/JP270538. [17] Ortiz A, Mattace-Raso F, Soler MJ, et al. Ageing meets kidney disease[J]. Nephrol Dial Transplant, 2023, 38(3): 523-526. DOI: 10.1093/ndt/gfac199. [18] Murray CJ, Barber RM, Foreman KJ, et al. Global, regional, and national disability-adjusted life years (DALYs) for 306 diseases and injuries and healthy life expectancy (HALE) for 188 countries, 1990-2013: quantifying the epidemiological transition[J]. Lancet, 2015, 386(10009): 2145-2191. DOI: 10.1016/s0140-6736(15)61340-X. [19] Burris JC, Werner CM, Woolf K. The relationship between dietary intake and dietary-focused lifestyle interventions on risk factors associated with cardiovascular disease in firefighters[J]. Curr Nutr Rep, 2022, 11(2): 206-224. DOI: 10.1007/s13668-022-00406-3. [20] Levin MG, Klarin D, Assimes TL, et al. Genetics of smoking and risk of atherosclerotic cardiovascular diseases: a Mendelian randomization study[J]. JAMA Netw Open, 2021, 4(1): e2034461. DOI: 10.1001/jamanetworkopen.2020.34461. [21] De Bont J, Jaganathan S, Dahlquist M, et al. Ambient air pollution and cardiovascular diseases: an umbrella review of systematic reviews and meta-analyses[J]. J Intern Med, 2022, 291(6): 779-800. DOI: 10.1111/joim.13467. [22] Lv S, Shen Z, Zhang H, et al. Association between exposure to the Chinese famine during early life and the risk of chronic kidney disease in adulthood[J]. Environ Res, 2020, 184: 109312. DOI: 10.1016/j.envres.2020.109312. -

 点击查看大图
点击查看大图

计量
- 文章访问数: 111
- HTML全文浏览量: 28
- PDF下载量: 47
- 被引次数: 0