

A cohort study of the effect of cumulative exposure to LDL-C on cardiovascular disease among the uyghur population in southern Xinjiang
-
摘要:
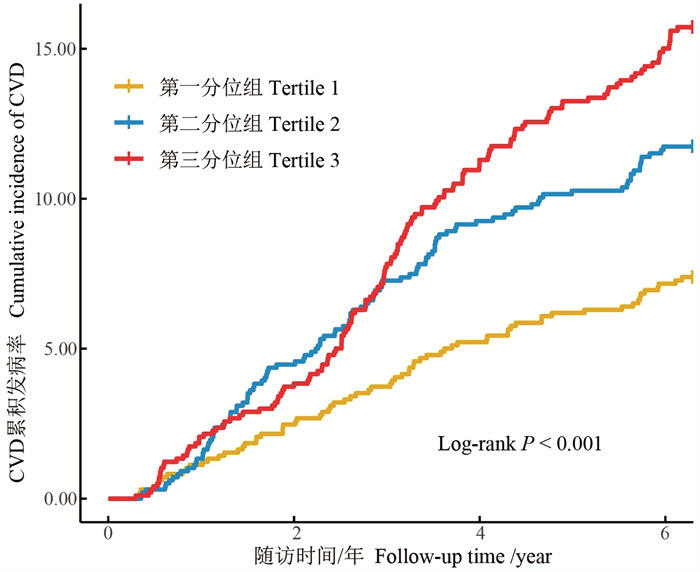
目的 探讨新疆维吾尔自治区(简称新疆)南疆维吾尔族人群中低密度脂蛋白胆固醇(low density lipoprotein cholesterol, LDL-C)累积暴露对心血管病(cardiovascular diseases, CVD)的影响。 方法 研究队列来自新疆生产建设兵团第三师五十一团,纳入在2016-2022年调查期间有3次LDL-C测量值,且相邻两次测量时间间隔≥2年的2 950名维吾尔族人群作为研究对象。使用每个时间间隔LDL-C测量值的加权和(值×时间)计算LDL-C累积暴露(cumulative low density lipoprotein cholesterol, cumLDL-C)。按cumLDL-C三分位数分组,采用Log-rank检验比较各组CVD累积发病率的差异; 使用Cox比例风险回归模型分析cumLDL-C对发生CVD的影响。 结果 随访期间共新发CVD事件322例(10.92%),cumLDL-C第一、二、三分位组CVD累积发病率分别为7.12%、11.08%、14.55%,经Log-rank检验,差异有统计学意义($ \begin{equation}\chi^2\end{equation}$=27.440, P < 0.001)。Cox比例风险回归模型显示,校正多种混杂因素后,与cumLDL-C第一分位组相比,cumLDL-C第三分位组发生CVD的HR=1.51(95% CI: 1.12~2.06);cumLDL-C每增加一个标准差,发生CVD的风险增加14%(HR=1.14, 95% CI: 1.01~1.28)。 结论 在新疆南疆维吾尔族人群中,高LDL-C累积暴露是该人群发生CVD的独立危险因素,长期保持较低的LDL-C水平,有助于降低该人群CVD的发生风险。 Abstract:Objective To explore the effect of cumulative exposure to low-density lipoprotein cholesterol (LDL-C) on cardiovascular disease (CVD) among the Uyghur population in southern Xinjiang. Methods We recruited 2 950 Uyghurs from the 51st Corps of the 3rd division of Xinjiang Production and Construction Corps, who had measured LDL-C at least three times during the 2016-2022 survey period, and two adjacent measurement intervals ≥2 years. Cumulative LDL-C (cumLDL-C) exposure was calculated by the weighted sum of LDL-C measured value for each time interval (value × time). Participants were grouped according to the cumLDL-C tertiles. The Log-rank test was used to compare the differences in the cumulative incidence of CVD among the groups. Cox proportional hazard regression models were used to estimate the effect of cumLDL-C on CVD. Results During the follow-up period, 322(10.92%) CVD events occurred. The cumulative incidence of CVD from the first to third tertile group of cumLDL-C was 7.12%, 11.08%, and 14.55%, respectively ($ \begin{equation}\chi^2\end{equation}$=27.440, P < 0.001). Cox proportional hazards model showed that after adjusting for multiple confounders, the risk of CVD in the third tertile of cumLDL-C compared with the first tertile was 1.51 times higher (HR=1.51, 95% CI: 1.12-2.06). Each standard deviation increase in cumLDL-C was associated with a 14% increased risk of CVD (HR=1.14, 95% CI: 1.01-1.28). Conclusions In the Uyghur population in southern Xinjiang, cumulative exposure to high LDL-C is an independent risk factor for CVD, and maintaining low LDL-C levels for a long period of time can help reduce the risk of CVD in this population. -

图 1 cumLDL-C各组CVD累积发病率
CVD: 心血管病; cumLDL-C: 低密度脂蛋白胆固醇累积暴露。
Figure 1. Incidence rate of CVD by tertile of cumLDL-C
CVD: cardiovascular disease; cumLDL-C: cumulative low density lipoprotein cholesterol.

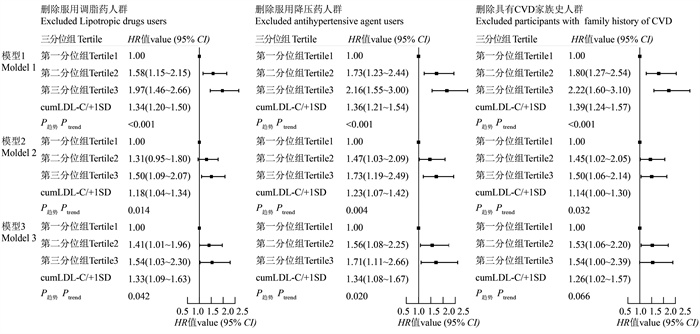
图 2 cumLDL-C影响CVD的多因素Cox回归模型(敏感性分析)
CVD:心血管病; cumLDL-C:低密度脂蛋白胆固醇累积暴露; 模型1:以是否发生CVD为因变量,以cumLDL-C三分位组(以第一分位组为对照组)为自变量;模型2:在模型1的基础上校正年龄、性别、BMI、基线收缩压、基线舒张压、吸烟、文化程度、总胆固醇、三酰甘油、高密度脂蛋白胆固醇、空腹血糖;模型3:在模型1的基础上校正基线LDL-C。
Figure 2. Multifactorial Cox regression model for the effect of cumLDL-C on CVD (sensitivity analysis)
CVD: cardiovascular disease; cumLDL-C: cumulative low density lipoprotein cholesterol; Model 1: the occurrence of CVD as the dependent variable and the cumLDL-C tertile group (with tertile 1 as the reference) as the independent variable; Model 2: adjusted for age, gender, BMI, baseline systolic blood pressure, baseline diastolic blood pressure, smoking, education, total cholesterol, triglycerides, high-density lipoprotein cholesterol, and fasting plasma glucose based on model 1; Model 3: adjusted for baseline LDL-C based on model 1.
表 1 cumLDL-C三分位组研究对象的基线特征
Table 1. Baseline characteristics of participants by tertile of cumLDL-C
变量
VariablecumLDL-C三分位组 总人群 ①
Total ①
(n=2 950)F/$ \begin{equation} \chi^2 \end{equation}$
值valueP值
value第一分位组 ① Tertile 1 ① (n=983) 第二分位组 ① Tertile 2 ① (n=984) 第三分位组 ① Tertile 3 ① (n=983) 年龄/岁Age/years 42.58±12.22 46.48±11.87② 47.85±11.84②,③ 45.64±12.18 51.237 < 0.001 男性Male 420(42.73) 466(47.36) 453(46.08) 1339(45.39) 4.541 0.103 BMI/(kg·m-2) 25.77±4.63 26.37±4.61② 27.04±4.59②,③ 26.40±4.64 18.735 < 0.001 SBP/mmHg 125.59±18.12 128.40±19.19② 130.22±20.06② 128.07±19.23 14.567 < 0.001 DBP/mmHg 74.17±11.48 74.96±11.56 76.11±12.35② 75.08±11.83 6.695 0.001 cumLDL-C/(mmol·L-1·年-1) 9.70±2.52 14.25±0.93② 18.93±2.79②,③ 14.29±4.38 4 196.084 < 0.001 吸烟Smoking 187(19.02) 226(22.97) 215(21.87) 628(21.29) 4.865 0.088 饮酒Drinking 50(5.09) 67(6.81) 76(7.73) 193(6.54) 5.795 0.055 文化程度Education 50.170 < 0.001 文盲及半文盲Illiteracy and semi-illiteracy 363(36.93) 465(47.26)② 473(48.12)②,③ 1 301(44.10) 小学Primary school 296(30.11) 281(28.56) 293(29.81) 870(29.49) 初中Junior high school 257(26.14) 168(17.07) 155(15.77) 580(19.66) 高中及以上Senior high school and above 67(6.82) 70(7.11) 62(6.31) 199(6.75) TC/(mmol·L-1) 4.25±1.29 4.69±0.86② 5.25±1.27②,③ 4.73±1.23 184.657 < 0.001 TG/(mmol·L-1) 1.59±1.44 1.74±1.36 1.90±1.60②,③ 1.74±1.48 10.992 < 0.001 HDL-C/(mmol·L-1) 1.60±0.69 1.46±0.54② 1.39±0.52②,③ 1.48±0.60 32.536 < 0.001 LDL-C/(mmol·L-1) 1.86±0.69 2.61±0.49② 3.44±0.75②,③ 2.64±0.92 1 431.809 < 0.001 FPG/(mmol·L-1) 4.95±1.90 4.97±2.09 5.24±2.96②,③ 5.06±2.37 4.764 0.009 血脂异常Dyslipidaemic 260(26.45) 352(35.77)② 522(53.10)②,③ 1 134(38.44) 151.991 < 0.001 服用调脂药Lipotropic drugs users 12(1.22) 21(2.13) 39(3.97)②,③ 72(2.44) 16.155 < 0.001 服用降压药Antihypertensive agent users 39(3.97) 48(4.88) 70(7.12)② 157(5.32) 10.279 0.006 CVD家族史Family history of CVD 136(13.84) 150(15.24) 187(19.02)② 473(16.03) 10.511 0.005 CVD事件CVD events 70(7.12) 109(11.08)② 143(14.55)②,③ 322(10.92) 27.915 < 0.001 随访时间Follow-up time 6.05±0.98 5.89±1.25② 5.82±1.29② 5.92±1.18 9.644 < 0.001 注:cumLDL-C,低密度脂蛋白胆固醇累积暴露;SBP,基线收缩压;DBP,基线舒张压;TC,总胆固醇;TG,三酰甘油;HDL-C,高密度脂蛋白胆固醇;LDL-C,低密度脂蛋白胆固醇;FPG,空腹血糖;CVD,心血管病。
①以人数(占比/%)或x±s表示;②与第一分位组相比,P < 0.05;③与第二分位组相比,P < 0.05。
Note: cumLDL-C, cumulative low density lipoprotein cholesterol; SBP, baseline systolic blood pressure; DBP, baseline diastolic blood pressure; TC, total cholesterol; TG, triglycerides; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; FPG, fasting plasma glucose; CVD, cardiovascular disease.
① Number of people (proportion/%) or x±s; ② compared with tertile 1, P < 0.05; ③ compared with tertile 2, P<0.05. 下载: 导出CSV
下载: 导出CSV
表 2 cumLDL-C影响CVD的多因素Cox回归模型
Table 2. Multifactorial Cox regression model for the effect of cumLDL-C on CVD
组别Groups 模型1 Model 1 HR值value (95% CI) 模型2 Model 2 HR值value (95% CI) 模型3 Model 3 HR值value (95% CI) 第一分位组Tertile 1 1.00 1.00 1.00 第二分位组Tertile 2 1.60(1.18~2.16) 1.33(0.98~1.81) 1.44(1.05~1.99) 第三分位组Tertile 3 2.12(1.59~2.82) 1.51(1.12~2.06) 1.69(1.16~2.48) cumLDL-C/+1SD 1.36(1.22~1.51) 1.14(1.01~1.28) 1.33(1.10~1.61) P趋势 Ptrend < 0.001 0.009 0.008 基线LDL-C Baseline LDL-C 1.32(1.18~1.47) 1.16(1.06~1.33) 注:1. cumLDL-C,低密度脂蛋白胆固醇累积暴露; CVD,心血管病;LDL-C,低密度脂蛋白胆固醇。
2. 模型1,以是否发生CVD为因变量,以cumLDL-C三分位组(以第一分位组为对照组)为自变量;模型2,在模型1的基础上校正年龄、性别、BMI、基线收缩压、基线舒张压、吸烟、文化程度、总胆固醇、三酰甘油、高密度脂蛋白胆固醇、空腹血糖;模型3,在模型1的基础上校正基线LDL-C。
Note: 1. cumLDL-C, cumulative low density lipoprotein cholesterol; CVD, cardiovascular disease; LDL-C, low density lipoprotein cholesterol.
2. Model 1, the occurrence of CVD as the dependent variable and the cumLDL-C tertile group (with tertile 1 as the reference) as the independent variable; Model 2, adjusted for age, gender, BMI, baseline systolic blood pressure, baseline diastolic blood pressure, smoking, education, total cholesterol, triglycerides, high-density lipoprotein cholesterol, and fasting plasma glucose based on model 1; Model 3, adjusted for baseline LDL-C based on model 1.
下载: 导出CSV
-
[1] Roth GA, Mensah GA, Johnson CO, et al. Global burden of cardiovascular diseases and risk factors, 1990-2019: update from the GBD 2019 study[J]. J Am Coll Cardiol, 2020, 76(25): 2982-3021. DOI: 10.1016/j.jacc.2020.11.010. [2] 中国心血管健康与疾病报告编写组. 中国心血管健康与疾病报告2022概要[J]. 中国循环杂志, 2023, 38(6): 583-612. DOI: 10.3969/j.issn.1000-3614.2023.06.001.The Writing Committee of the Report on Cardiovascular Health and Diseases in China. Report on cardiovascular health and diseases in China 2022: an updated summary[J]. Chin Circul J, 2023, 38(6): 583-612. DOI: 10.3969/j.issn.1000-3614.2023.06.001. [3] Grundy SM, Stone NJ, Bailey AL, et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA guideline on the management of blood cholesterol: a report of the american college of cardiology/american heart association task force on clinical practice guidelines[J]. Circulation, 2019, 139(25). DOI: 10.1161/CIR.0000000000000625. [4] 张梦妮, 李茂婷, 职心乐, 等. 1990-2019年中国动脉粥样硬化心血管病疾病负担变化及其危险因素分析[J]. 中华流行病学杂志, 2021, 42(10): 1797-1803. DOI: 10.3760/cma.j.cn112338-20201208-01390.Zhang MN, Li MT, Zhi XL, et al. Trends of a burden on atherosclerotic cardiovascular disease and its related risk factors in China, 1990 to 2019[J]. Chin J Epidemiol, 2021, 42(10): 1797-1803. DOI: 10.3760/cma.j.cn112338-20201208-01390. [5] Baigent C, Blackwell L, Emberson J, et al. Efficacy and safety of more intensive lowering of LDL cholesterol: a meta-analysis of data from 170 000 participants in 26 randomised trials[J]. Lancet, 2010, 376(9753): 1670-1681. DOI: 10.1016/S0140-6736(10)61350-5. [6] Domanski MJ, Tian X, Wu CO, et al. Time course of LDL cholesterol exposure and cardiovascular disease event risk[J]. J Am Coll Cardiol, 2020, 76(13): 1507-1516. DOI: 10.1016/j.jacc.2020.07.059. [7] Duncan MS, Vasan RS, Xanthakis V. Trajectories of blood lipid concentrations over the adult life course and risk of cardiovascular disease and all-cause mortality: observations from the framingham study over 35 years[J]. J Am Heart Assoc, 2019, 8(11). DOI: 10.1161/JAHA.118.011433. [8] Ference BA, Graham I, Tokgozoglu L, et al. Impact of lipids on cardiovascular health: JACC health promotion series[J]. J Am Coll Cardiol, 2018, 72(10): 1141-1156. DOI: 10.1016/j.jacc.2018.06.046. [9] Ference BA, Majeed F, Penumetcha R, et al. Effect of naturally random allocation to lower low-density lipoprotein cholesterol on the risk of coronary heart disease mediated by polymorphisms in NPC1L1, HMGCR, or both[J]. J Am Coll Cardiol, 2015, 65(15): 1552-1561. DOI: 10.1016/j.jacc.2015.02.020. [10] Centers For Disease Control And Prevention CDC. Cigarette smoking among adults--United States, 1992, and changes in the definition of current cigarette smoking[J]. MMWR Morb Mortal Wkly Rep, 1994, 43(19): 342-346. [11] Sun K, Ren M, Liu D, et al. Alcohol consumption and risk of metabolic syndrome: a meta-analysis of prospective studies[J]. Clin Nutr, 2014, 33(4): 596-602. DOI: 10.1016/j.clnu.2013.10.003. [12] 来雪峰. 血尿酸和胆红素及其变化与心血管疾病发生风险的前瞻性队列研究[D]. 武汉: 华中科技大学, 2021.Lai XF. Associations of serum uric acid, bilirubin and their change with risk of incident cardiovascular disease in a prospective cohort study[D]. Wuhan: Huazhong University of Science and Technology, 2021. [13] 诸骏仁, 高润霖, 赵水平, 等. 中国成人血脂异常防治指南(2016年修订版)[J]. 中国循环杂志, 2016, 31(10): 937-953. DOI: 10.3969/j.issn.1000-3614.2016.10.001.Zhu JR, Gao RL, Zhao SP, et al. Chinese guidelines for prevention and control of dyslipidemia in adults (2016 Revision)[J]. Chin Circul J, 2016, 31(10): 937-953. DOI: 10.3969/j.issn.1000-3614.2016.10.001. [14] 宋永健, 杜鑫, 郑梦伊, 等. 低密度脂蛋白胆固醇累积暴露对新发急性心肌梗死影响的前瞻性队列研究[J]. 中国循环杂志, 2020, 35(3): 246-253. DOI: 10.3969/j.issn.1000-3614.2020.03.004.Song YJ, Du X, Zheng MY, et al. A prospective cohort study of the effect of cumulative exposure to low density lipoprotein cholesterol on new-onset acute myocardial infarction[J]. Chin Circul J, 2020, 35(3): 246-253. DOI: 10.3969/j.issn.1000-3614.2020.03.004. [15] Zhang Y, Pletcher MJ, Vittinghoff E, et al. Association between cumulative low-density lipoprotein cholesterol exposure during young adulthood and middle age and risk of cardiovascular events[J]. JAMA Cardiol, 2021, 6(12): 1406. DOI: 10.1001/jamacardio.2021.3508. [16] Mo J, Chen Z, Xu J, et al. The impact of the cumulative burden of LDL-C and hs-CRP on cardiovascular risk: a prospective, population-based study[J]. Aging (Albany NY), 2020, 12(12): 11990-12001. DOI: 10.18632/aging.103365. [17] Goldstein JL, Brown MS. A century of cholesterol and coronaries: from plaques to genes to statins[J]. Cell, 2015, 161(1): 161-172. DOI: 10.1016/j.cell.2015.01.036. [18] Ference BA, Ginsberg HN, Graham I, et al. Low-density lipoproteins cause atherosclerotic cardiovascular disease. 1. Evidence from genetic, epidemiologic, and clinical studies. a consensus statement from the european atherosclerosis society consensus panel[J]. Eur Heart J, 2017, 38(32): 2459-2472. DOI: 10.1093/eurheartj/ehx144. [19] 中国心血管健康与疾病报告编写组. 中国心血管健康与疾病报告2020概要[J]. 中国循环杂志, 2021, 36(6): 521-545. DOI: 10.3969/j.issn.1000-3614.2021.06.001.The Writing Committee of the Report on Cardiovascular Health and Diseases in China. Report on cardiovascular health and diseases in China 2020: an updated summary[J]. Chin Circul J, 2021, 36(6): 521-545. DOI: 10.3969/j.issn.1000-3614.2021.06.001. [20] 曾雨虹, 刘静, 刘军, 等. 超高危ASCVD患者的界定标准对住院ACS患者降脂治疗需求的影响[J]. 中华心血管病杂志, 2020, 48(12): 1039-1046. DOI: 10.3760/cma.j.cn112148-20200710-00549.Zeng YH, Liu J, Liu J, et al. The expanding needs on lipid-lowering treatment in patients with acute coronary syndrome by applying newly issued definition of extreme high-risk by Chinese society of cardiology[J]. Chin J Cardiol, 2020, 48(12): 1039-1046. DOI: 10.3760/cma.j.cn112148-20200710-00549. [21] Vallejo-Vaz AJ, Robertson M, Catapano AL, et al. Low-density lipoprotein cholesterol lowering for the primary prevention of cardiovascular disease among men with primary elevations of low-density lipoprotein cholesterol levels of 190 mg/dL or above: analyses from the WOSCOPS (West of Scotland Coronary Prevention Study) 5-year randomized trial and 20-year observational follow-up[J]. Circulation, 2017, 136(20): 1878-1891. DOI: 10.1161/CIRCULATIONAHA.117.027966. [22] Sever PS, Chang CL, Gupta AK, et al. The anglo-scandinavian cardiac outcomes trial: 11-year mortality follow-up of the lipid-lowering arm in the U. K[J]. Eur Heart J, 2011, 32(20): 2525-2532. DOI: 10.1093/eurheartj/ehr333. [23] LIPID Study Group Long-term Intervention With Pravastatin In Ischaemic Disease. Long-term effectiveness and safety of pravastatin in 9014 patients with coronary heart disease and average cholesterol concentrations: the LIPID trial follow-up[J]. Lancet, 2002, 359(9315): 1379-1387. DOI: 10.1016/S0140-6736(02)08351-4. [24] 王宇翔, 马儒林, 郭恒, 等. 新疆农村地区维吾尔族人群心血管疾病患病率及其影响因素[J]. 中华疾病控制杂志, 2023, 27(4): 385-391. DOI: 10.16462/j.cnki.zhjbkz.2023.04.003.Wang YX, Ma RL, Guo H, et al. Prevalence of cardiovascular disease and its influencing factors among the Uygur population in rural areas of Xinjiang[J]. Chin J Dis Control Prev, 2023, 27(4): 385-391. DOI: 10.16462/j.cnki.zhjbkz.2023.04.003. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 69
- HTML全文浏览量: 13
- PDF下载量: 9
- 被引次数: 0