

A systematic review of Mendelian randomization for behavioral and nutrient-related factors of intracranial aneurysm
-
摘要:
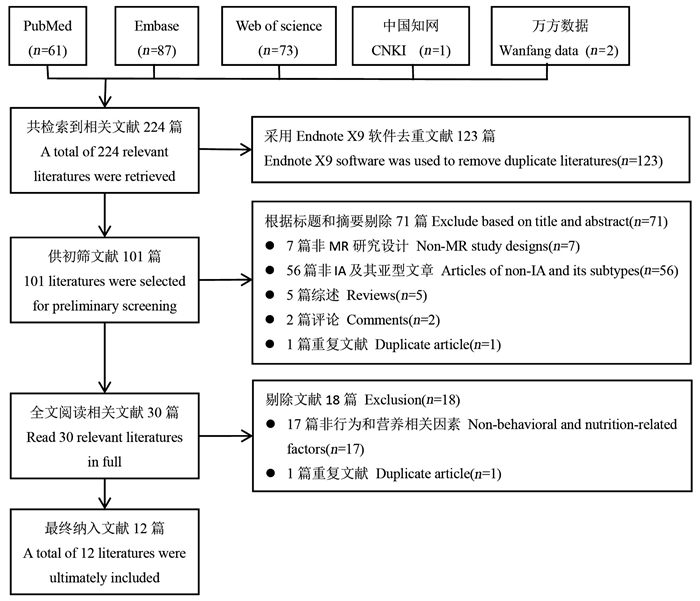
目的 通过总结孟德尔随机化(Mendelian randomization, MR)研究的证据来评估行为和营养相关因素与颅内动脉瘤(intracranial aneurysm, IA)的关联,为进一步阐明IA的病因和发病机制提供线索。 方法 系统检索PubMed、Embase、Web of Science、中国知网和万方数据知识服务平台等中英文数据库,筛选出行为和营养相关因素与IA关联的MR研究,采用叙述整合的方法将纳入文献归类,进行定性系统综述。 结果 共纳入2018–2023年发表的12篇文献,其中4篇被判定为高质量研究。这些研究探讨了吸烟、咖啡摄入、体力活动、饮酒和饮茶等行为因素及同型半胱氨酸、血清镁、血清铁、血清钙、多不饱和脂肪酸等营养因素与IA及其亚型的关系,但存在重复发表的问题。4项基于同一欧洲人群、不同工具变量筛选标准的MR研究均支持吸烟是IA及其亚型的危险因素;关于咖啡摄入、体力活动、同型半胱氨酸、血清镁、血清钙与IA及其亚型的关联结果不同;各有1项MR研究提示血清铁和多不饱和脂肪酸与IA及其亚型存在关联。 结论 吸烟增加IA及其亚型发病风险,对于其他行为和营养相关因素与IA及其亚型的关联需要进一步地深入研究。MR研究本身存在局限性,需综合其他证据,谨慎进行因果推断。 Abstract:Objective To evaluate the association between behavioral and nutrient-related factors and intracranial aneurysm (IA) by summarizing evidences from Mendelian randomization (MR) studies for further elucidating the etiology and pathogenesis of IA. Methods PubMed, Embase, Web of Science, CNKI and Wanfang were systematically searched to screen out related studies. The included literatures were classified by narrative integration method for qualitative systematic review. Results A total of 12 studies published between 2018 and 2023 were included, of which 4 were judged to be of high quality. These studies explored the relationship between behavior (smoking, coffee intake, physical activity, alcohol and tea consumption) and nutrition-related factors (homocysteine, serum magnesium, serum iron, serum calcium, and polyunsaturated fatty acids) and IA and its subtypes, but they had the problem of being published repeatedly. Four MR studies based on different instrumental variables screening criteria in the same european population all supported smoking as a risk factor for IA and its subtypes; the results regarding coffee intake, physical activity, homocysteine, serum magnesium, and serum calcium were discrepancy. One MR study each suggested that serum iron and polyunsaturated fatty acids were associated with IA and its subtypes. Conclusions Smoking can increase the risk of IA and its subtypes, the association of other behavioral and nutrient-related factors with IA and its subtypes needs further investigation. The MR study itself has limitations, which requires careful causal inference based on other evidences. -

图 1 文献筛选流程
MR: 孟德尔随机化; IA: 颅内动脉瘤。
Figure 1. Literature screening flow chart
MR: Mendelian randomization; IA: intracranial aneurysm.
表 1 行为因素与IA及其亚型MR研究的主要信息
Table 1. Main information of MR studies on behavioral factors and IA and its subtypes
暴露
Exposure作者(年份)
Author (year)暴露相关信息
Exposure related information结局相关信息
Outcome related information来源(PMID)
Source (PMID)样本量
Sample size变量
Variable来源(PMID)
Source
(PMID)样本量Sample size 病例
Case对照
Control吸烟Smoking Karhunen V[8](2021) 30643251 1 232 091 IA 33199917 7 495 71 934 Sun XH[10](2022) 30643251 1 232 091 IA 33199917 7 495 71 934 Tian DY[9](2022) 30643251 1 232 091 IA 33199917 7 495 71 934 Zeng CD[7](2023) 30643251 1 232 091 IA 33199917 7 495 71 934 Karhunen V[8](2021) 30643251 1 232 091 aSAH 33199917 5 140 71 934 Sun XH[10](2022) 30643251 1 232 091 aSAH 33199917 5 140 71 934 Acosta JN[17](2022) UKB 132 566 aSAH UKB 904 131 662 Tian DY[9](2022) 30643251 1 232 091 aSAH 33199917 5 140 71 934 Zeng CD[7](2023) 30643251 1 232 091 aSAH 33199917 5 140 71 934 Sun XH[10](2022) 30643251 1 232 091 uIA 33199917 2 070 71 934 Tian DY[9](2022) 30643251 1 232 091 uIA 33199917 2 070 71 934 Zeng CD[7](2023) 30643251 1 232 091 uIA 33199917 2 070 71 934 咖啡摄入Coffee consumption Karhunen V[8](2021) 31046077 375 833 IA 33199917 7 495 71 934 Sun XH[10](2022) 25288136 121 524 IA 33199917 7 495 71 934 Zhang ZZ[11](2023) 25288136 121 524 IA 33199917 7 495 71 934 Karhunen V[8](2021) 31046077 375 833 aSAH 33199917 5 140 71 934 Sun XH[10](2022) 25288136 121 524 aSAH 33199917 5 140 71 934 Zhang ZZ[11](2023) 25288136 121 524 aSAH 33199917 5 140 71 934 Sun XH[10](2022) 25288136 121 524 uIA 33199917 2 070 71 934 Zhang ZZ[11](2023) 25288136 121 524 uIA 33199917 2 070 71 934 体力活动Physical activity Karhunen V[8](2021) 29899525 377 234 IA 33199917 7 495 71 934 Sun XH[10](2022) 29899525 377 234 IA 33199917 7 495 71 934 Tian DY[9](2022) 29899525 377 234 IA 33199917 7 495 71 934 Karhunen V[8](2021) 29899525 377 234 aSAH 33199917 5 140 71 934 Sun XH[10](2022) 29899525 377 234 aSAH 33199917 5 140 71 934 Sun XH[10](2022) 29899525 377 234 uIA 33199917 2 070 71 934 饮酒Drinking 刘新志[16](2018)
Liu XZ[16](2018)①湘雅医院
Xiangya hospital846 IA 湘雅医院
Xiangya hospital421 425 Sun XH[10](2022) 30643251 1 232 091 IA 33199917 7 495 71 934 Tian DY[9](2022) 30643251 1 232 091 IA 33199917 7 495 71 934 Sun XH[10](2022) 30643251 1 232 091 aSAH 33199917 5 140 71 934 Sun XH[10](2022) 30643251 1 232 091 uIA 33199917 2 070 71 934 饮茶Tea consumption Zhang ZZ[11](2023) UKB 349 376 IA 33199917 7 495 71 934 Zhang ZZ[11](2023) UKB 349 376 aSAH 33199917 5 140 71 934 Zhang ZZ[11](2023) UKB 349 376 uIA 33199917 2 070 71 934 暴露
Exposure第一作者(年份)
First author (year)筛选标准Screening criteria IVW OR值value
(95% CI)质量评分
Quality scoreP值value r2值value F值value 吸烟Smoking Karhunen V[8](2021) < 5×10-8 <0.01 — 1.85(1.50~2.29) 7 Sun XH[10](2022) < 5×10-8 <0.1 >10 1.56(1.38~1.75) 5 Tian DY[9](2022) < 5×10-8 <0.01 >10 1.53(1.32~1.77) 5 Zeng CD[7](2023) < 5×10-8 <0.001 >10 1.89(1.49~2.41) 6 Karhunen V[8](2021) < 5×10-8 <0.01 — 1.62(1.24~2.13) 7 Sun XH[10](2022) < 5×10-8 <0.1 >10 1.46(1.27~1.68) 5 Acosta JN[17](2022) < 5×10-8 <0.1 — 1.57(1.13~2.17) 7 Tian DY[9](2022) < 5×10-8 <0.01 >10 1.72(1.41~2.10) 5 Zeng CD[7](2023) < 5×10-8 <0.001 >10 1.83(1.39~2.42) 6 Sun XH[10](2022) < 5×10-8 <0.1 >10 1.90(1.57~2.31) 5 Tian DY[9](2022) < 5×10-8 <0.01 >10 2.54(1.93~3.35) 5 Zeng CD[7](2023) < 5×10-8 <0.001 >10 2.18(1.46~3.25) 6 咖啡摄入Coffee consumption Karhunen V[8](2021) < 5×10-8 <0.01 — 0.83(0.49~1.40) 7 Sun XH[10](2022) < 5×10-8 <0.1 >10 1.12(0.67~1.85) 5 Zhang ZZ[11](2023) < 5×10-8 <0.1 — 1.42(1.09~1.86) 6 Karhunen V[8](2021) < 5×10-8 <0.01 — 1.00(0.53~1.91) 7 Sun XH[10](2022) < 5×10-8 <0.1 >10 1.16(0.66~2.02) 5 Zhang ZZ[11](2023) < 5×10-8 <0.1 — 1.51(1.13~2.03) 6 Sun XH[10](2022) < 5×10-8 <0.1 >10 1.09(0.59~2.00) 5 Zhang ZZ[11](2023) < 5×10-8 <0.1 — 1.20(0.74~1.96) 6 体力活动Physical activity Karhunen V[8](2021) < 5×10-8 <0.01 — 0.22(0.03~1.50) 7 Sun XH[10](2022) < 5×10-8 <0.1 >10 0.26(0.07~0.94) 5 Tian DY[9](2022) < 5×10-8 <0.01 >10 0.41(0.11~1.45) 5 Karhunen V[8](2021) < 5×10-8 <0.01 — 0.05(0.01~0.47) 7 Sun XH[10](2022) < 5×10-8 <0.1 >10 0.14(0.03~0.60) 5 Sun XH[10](2022) < 5×10-8 <0.1 >10 0.80(0.08~7.94) 5 饮酒Drinking 刘新志[16](2018) Liu XZ[16](2018)① — — — 1.45(0.18~10.98) 4 Sun XH[10](2022) 5×10-8 <0.1 >10 1.56(0.74~3.31) 5 Tian DY[9](2022) 5×10-8 <0.01 >10 1.29(0.68~2.45) 5 Sun XH[10](2022) 5×10-8 <0.1 >10 1.51(0.71~3.21) 5 Sun XH[10](2022) 5×10-8 <0.1 >10 1.73(0.54~5.56) 5 饮茶Tea consumption Zhang ZZ[11](2023) 5×10-8 <0.1 — 1.18(0.95~1.48) 6 Zhang ZZ[11](2023) 5×10-8 <0.1 — 1.16(0.91~1.48) 6 Zhang ZZ[11](2023) 5×10-8 <0.1 — 1.26(0.92~1.72) 6 注:IA,颅内动脉瘤;MR,孟德尔随机化;aSAH,动脉瘤性蛛网膜下腔出血;uIA,未破裂颅内动脉瘤;UKB,英国生物银行;IVW,逆方差加权法;“—”表示数据无法获取。
①表示样本来自中国人群,其余都来自欧洲人群。
Note: IA, intracranial aneurysm; MR, Mendelian randomization; aSAH, aneurysmal subarachnoid hemorrhage; uIA, unruptured intracranial aneurysm; UKB, UK Biobank; IVW, inverse variance weighting method; "—" indicates that the data cannot be obtained.
① It means that the samples are from Chinese population, and the rest are from European population. 下载: 导出CSV
下载: 导出CSV
表 2 营养相关因素与IA及其亚型MR研究的主要信息
Table 2. Main information of MR studies on nutrient-related factors and IA and its subtypes
暴露
Exposure第一作者(年份)
First author (year)暴露相关信息
Exposure related information结局相关信息
Outcome related information来源(PMID)
Source (PMID)样本量
Sample size变量
Variable来源(PMID)
Source
(PMID)样本量Sample size 病例
Case对照
ControlHcy Ma CC[12](2022) 23824729 44 147 IA 33199917 7 495 71 934 Sun XH[10](2022) 23824729 44 147 IA 33199917 7 495 71 934 Wen ZH[13](2023) 23824729 44 147 IA 33199917 7 495 71 934 Ma CC[12](2022) 23824729 44 147 aSAH 33199917 5 140 71 934 Sun XH[10](2022) 23824729 44 147 aSAH 33199917 5 140 71 934 Ma CC[12](2022) 23824729 44 147 uIA 33199917 2 070 71 934 Sun XH[10](2022) 23824729 44 147 uIA 33199917 2 070 71 934 血清镁Magnesium Larsson SC[14](2021) 20700443 23 829 IA 33199917 7 495 71 934 Sun XH[10](2022) 20700443 15 366 IA 33199917 7 495 71 934 Larsson SC[14](2021) 20700443 23 829 aSAH 33199917 5 140 71 934 Sun XH[10](2022) 20700443 15 366 aSAH 33199917 5 140 71 934 Larsson SC[14](2021) 20700443 23 829 uIA 33199917 2 070 71 934 Sun XH[10](2022) 20700443 15 366 uIA 33199917 2 070 71 934 血清铁Serum iron Sun XH[10](2022) 25352340 48 972 IA 33199917 7 495 71 934 Sun XH[10](2022) 25352340 48 972 aSAH 33199917 5 140 71 934 Sun XH[10](2022) 25352340 48 972 uIA 33199917 2 070 71 934 血清钙Serum calcium Sun XH[10](2022) 24068962 61 079 IA 33199917 7 495 71 934 Sun XH[10](2022) 24068962 61 079 aSAH 33199917 5 140 71 934 Zhang ZZ[18](2023) 24068962 61 079 aSAH 33199917 5 140 71 934 Sun XH[10](2022) 24068962 61 079 uIA 33199917 2 070 71 934 ω3-PUFA Yu WJ[15](2023) 35692035 114 999 IA 33199917 6 252 59 544 DHA Yu WJ[15](2023) 35692035 114 999 IA 33199917 6 252 59 544 ω3-PUFA/总脂肪ω3-PUFA/total fat Yu WJ[15](2023) 35692035 114 999 IA 33199917 6 252 59 544 ω6/ω3-PUFA Yu WJ[15](2023) 35692035 114 999 IA 33199917 6 252 59 544 ω3-PUFA Yu WJ[15](2023) 35692035 114 999 IA 33199917 6 252 59 544 ω6-PUFA Yu WJ[15](2023) 35692035 114 999 aSAH 33199917 4 196 59 544 DHA Yu WJ[15](2023) 35692035 114 999 aSAH 33199917 4 196 59 544 ω3-PUFA/总脂肪ω3-PUFA/total fat Yu WJ[15](2023) 35692035 114 999 aSAH 33199917 4 196 59 544 ω6/ω3-PUFA Yu WJ[15](2023) 35692035 114 999 aSAH 33199917 4 196 59 544 ω6-PUFA Yu WJ[15](2023) 35692035 114 999 aSAH 33199917 4 196 59 544 叶酸Folic acid Sun XH[10](2022) 23754956 37 341 IA 33199917 7 495 71 934 Sun XH[10](2022) 23754956 37 341 aSAH 33199917 5 140 71 934 Sun XH[10](2022) 23754956 37 341 uIA 33199917 2 070 71 934 25-羟基维生素D 25-hydroxyvitamin D Sun XH[10](2022) 32059762 401 460 IA 33199917 7 495 71 934 Tian DY[9](2022) 29343764 79 366 IA 33199917 7 495 71 934 Sun XH[10](2022) 32059762 401 460 aSAH 33199917 5 140 71 934 Zhang ZZ[18](2023) 29343764 79 366 aSAH 33199917 5 140 71 934 Sun XH[10](2022) 32059762 401 460 uIA 33199917 2 070 71 934 维生素A Vitamin A Sun XH[10](2022) 21878437 5 006 IA 33199917 7 495 71 934 Tian DY[9](2022) 21878437 5 006 IA 33199917 7 495 71 934 Sun XH[10](2022) 21878437 5 006 aSAH 33199917 5 140 71 934 Sun XH[10](2022) 21878437 5 006 uIA 33199917 2 070 71 934 维生素B6 Vitamin B6 Sun XH[10](2022) 19303062 1 864 IA 33199917 7 495 71 934 Sun XH[10](2022) 19303062 1 864 aSAH 33199917 5 140 71 934 Sun XH[10](2022) 19303062 1 864 uIA 33199917 2 070 71 934 维生素B12 Vitamin B12 Sun XH[10](2022) 23754956 45 576 IA 33199917 7 495 71 934 Tian DY[9](2022) 19744961 3 340 IA 33199917 7 495 71 934 Sun XH[10](2022) 23754956 45 576 aSAH 33199917 5 140 71 934 Sun XH[10](2022) 23754956 45 576 uIA 33199917 2 070 71 934 硒Selenium Sun XH[10](2022) 23720494 2 603 IA 33199917 7 495 71 934 Sun XH[10](2022) 23720494 2 603 aSAH 33199917 5 140 71 934 Sun XH[10](2022) 23720494 2 603 uIA 33199917 2 070 71 934 铜Copper Sun XH[10](2022) 23720494 2 603 IA 33199917 7 495 71 934 Sun XH[10](2022) 23720494 2 603 aSAH 33199917 5 140 71 934 Sun XH[10](2022) 23720494 2 603 uIA 33199917 2 070 71 934 锌Zinc Sun XH[10](2022) 23720494 2 603 IA 33199917 7 495 71 934 Sun XH[10](2022) 23720494 2 603 aSAH 33199917 5 140 71 934 Sun XH[10](2022) 23720494 2 603 uIA 33199917 2 070 71 934 暴露
Exposure第一作者(年份)
First author (year)筛选标准Screening criteria IVW OR值value
(95% CI)质量评分
Quality scoreP值value r2值value F值value Hcy Ma CC[12](2022) 5×10-8 <0.001 >10 1.12(0.92~1.37) 7 Sun XH[10](2022) 5×10-8 <0.1 >10 1.20(1.00~1.43) 5 Wen ZH[13](2023) 5×10-8 <0.01 — 1.38(1.07~1.79) 7 Ma CC[12](2022) 5×10-8 <0.001 >10 1.10(0.88~1.39) 7 Sun XH[10](2022) 5×10-8 <0.1 >10 1.21(0.98~1.49) 5 Ma CC[12](2022) 5×10-8 <0.001 >10 1.13(0.68~1.86) 7 Sun XH[10](2022) 5×10-8 <0.1 >10 1.09(0.71~1.66) 5 血清镁Magnesium Larsson SC[14](2021) 5×10-8 <0.6 — 0.66(0.49~0.91) 3 Sun XH[10](2022) 5×10-8 <0.1 >10 0.94(0.81~1.09) 5 Larsson SC[14](2021) 5×10-8 <0.6 — 0.67(0.48~0.92) 3 Sun XH[10](2022) 5×10-8 <0.1 >10 0.87(0.73~1.03) 5 Larsson SC[14](2021) 5×10-8 <0.6 — 0.57(0.30~1.06) 3 Sun XH[10](2022) 5×10-8 <0.1 >10 1.29(0.98~1.68) 5 血清铁Serum iron Sun XH[10](2022) 5×10-8 <0.1 >10 0.89(0.70~1.13) 5 Sun XH[10](2022) 5×10-8 <0.1 >10 0.78(0.61~0.99) 5 Sun XH[10](2022) 5×10-8 <0.1 >10 1.17(0.76~1.79) 5 血清钙Serum calcium Sun XH[10](2022) 5×10-8 <0.1 >10 1.48(0.61~3.61) 5 Sun XH[10](2022) 5×10-8 <0.1 >10 1.71(0.68~4.29) 5 Zhang ZZ[18](2023) 5×10-8 — — 1.96(1.00~3.81) 5 Sun XH[10](2022) 5×10-8 <0.1 >10 1.31(0.27~6.30) 5 ω3-PUFA Yu WJ[15](2023) 5×10-8 <0.001 >10 0.80(0.69~0.91) 6 DHA Yu WJ[15](2023) 5×10-8 <0.001 >10 0.75(0.63~0.87) 6 ω3-PUFA/总脂肪ω3-PUFA/total fat Yu WJ[15](2023) 5×10-8 <0.001 >10 0.80(0.71~0.90) 6 ω6/ω3-PUFA Yu WJ[15](2023) 5×10-8 <0.001 >10 1.27(1.12~1.44) 6 ω3-PUFA Yu WJ[15](2023) 5×10-8 <0.001 >10 0.78(0.57~1.06) 6 ω6-PUFA Yu WJ[15](2023) 5×10-8 <0.001 >10 0.71(0.61~0.84) 6 DHA Yu WJ[15](2023) 5×10-8 <0.001 >10 0.67(0.55~0.80) 6 ω3-PUFA/总脂肪ω3-PUFA/total fat Yu WJ[15](2023) 5×10-8 <0.001 >10 0.76(0.66~0.87) 6 ω6/ω3-PUFA Yu WJ[15](2023) 5×10-8 <0.001 >10 1.35(1.17~1.56) 6 ω6-PUFA Yu WJ[15](2023) 5×10-8 <0.001 >10 0.82(0.62~1.08) 6 叶酸Folic acid Sun XH[10](2022) 5×10-8 <0.1 >10 0.79(0.57~1.10) 5 Sun XH[10](2022) 5×10-8 <0.1 >10 0.76(0.52~1.12) 5 Sun XH[10](2022) 5×10-8 <0.1 >10 1.13(0.41~3.08) 5 25-羟基维生素D 25-hydroxyvitamin D Sun XH[10](2022) 5×10-8 <0.1 >10 0.98(0.79~1.21) 5 Tian DY[9](2022) 5×10-8 <0.01 >10 1.03(0.55~1.94) 5 Sun XH[10](2022) 5×10-8 <0.1 >10 1.00(0.77~1.28) 5 Zhang ZZ[18](2023) 5×10-8 — — 0.92(0.78~1.09) 5 Sun XH[10](2022) 5×10-8 <0.1 >10 0.91(0.65~1.29) 5 维生素A Vitamin A Sun XH[10](2022) 5×10-8 <0.1 >10 1.15(0.83~1.60) 5 Tian DY[9](2022) 5×10-8 <0.01 >10 1.03(0.78~1.37) 5 Sun XH[10](2022) 5×10-8 <0.1 >10 1.12(0.76~1.64) 5 Sun XH[10](2022) 5×10-8 <0.1 >10 1.02(0.55~1.92) 5 维生素B6 Vitamin B6 Sun XH[10](2022) 5×10-8 <0.1 >10 0.91(0.71~1.16) 5 Sun XH[10](2022) 5×10-8 <0.1 >10 1.01(0.77~1.34) 5 Sun XH[10](2022) 5×10-8 <0.1 >10 0.71(0.45~1.12) 5 维生素B12 Vitamin B12 Sun XH[10](2022) 5×10-8 <0.1 >10 1.00(0.85~1.19) 5 Tian DY[9](2022) 5×10-8 <0.01 >10 1.12(0.79~1.58) 5 Sun XH[10](2022) 5×10-8 <0.1 >10 1.05(0.86~1.28) 5 Sun XH[10](2022) 5×10-8 <0.1 >10 0.97(0.65~1.43) 5 硒Selenium Sun XH[10](2022) 5×10-8 <0.01 >10 0.94(0.81~1.09) 5 Sun XH[10](2022) 5×10-8 <0.1 >10 0.87(0.73~1.03) 5 Sun XH[10](2022) 5×10-8 <0.1 >10 1.29(0.98~1.68) 5 铜Copper Sun XH[10](2022) 5×10-8 <0.1 >10 1.00(0.85~1.19) 5 Sun XH[10](2022) 5×10-8 <0.1 >10 0.93(0.76~1.12) 5 Sun XH[10](2022) 5×10-8 <0.1 >10 1.20(0.88~1.64) 5 锌Zinc Sun XH[10](2022) 5×10-8 <0.1 >10 0.99(0.85~1.16) 5 Sun XH[10](2022) 5×10-8 <0.1 >10 1.03(0.87~1.23) 5 Sun XH[10](2022) 5×10-8 <0.1 >10 0.87(0.67~1.13) 5 注:IA,颅内动脉瘤;MR,孟德尔随机化;Hcy,同型半胱氨酸;ω3-PUFA,ω-3多不饱和脂肪酸;ω6-PUFA,ω-6多不饱和脂肪酸;aSAH,动脉瘤性蛛网膜下腔出血;uIA,未破裂颅内动脉瘤;IVW,逆方差加权法;“—”表示数据无法获取。
Note: IA, intracranial aneurysm; MR, Mendelian randomization; Hcy, homocysteine; ω3-PUFA, ω-3 polyunsaturated fatty acids; ω6-PUFA, ω-6 polyunsaturated fatty acids; aSAH, aneurysmal subarachnoid hemorrhage; uIA, unruptured intracranial aneurysm; IVW, inverse variance weighting method; "—" indicates that the data cannot be obtained.
下载: 导出CSV
-
[1] Vlak MH, Algra A, Brandenburg R, et al. Prevalence of unruptured intracranial aneurysms, with emphasis on sex, age, comorbidity, country, and time period: a systematic review and meta-analysis[J]. Lancet Neurol, 2011, 10(7): 626-636. DOI: 10.1016/S1474-4422(11)70109-0. [2] Rinkel GJ, Ruigrok YM. Preventive screening for intracranial aneurysms[J]. Int J Stroke, 2022, 17(1): 30-36. DOI: 10.1177/17474930211024584. [3] Ambekar S, Khandelwal P, Bhattacharya P, et al. Treatment of unruptured intracranial aneurysms: a review[J]. Expert Rev Neurother, 2016, 16(10): 1205-1216. DOI: 10.1080/14737175.2016.1199958. [4] Davis MC, Broadwater DR, Amburgy JW, et al. The clinical significance and reliability of self-reported smoking status in patients with intracranial aneurysms: a review[J]. Clin Neurol Neurosurg, 2015, 137: 44-49. DOI: 10.1016/j.clineuro.2015.06.016. [5] Czekajło A. Role of diet-related factors in cerebral aneurysm formation and rupture[J]. Rocz Panstw Zakl Hig, 2019, 70(2): 119-126. DOI: 10.32394/rpzh.2019.0061. [6] Haycock PC, Burgess S, Wade KH, et al. Best (but oft-forgotten) practices: the design, analysis, and interpretation of Mendelian randomization studies[J]. Am J Clin Nutr, 2016, 103(4): 965-978. DOI: 10.3945/ajcn.115.118216. [7] Zeng CD, Huang Z, Tao WG, et al. Genetically predicted tobacco consumption and risk of intracranial aneurysm: a Mendelian randomization study[J]. Environ Sci Pollut Res Int, 2023, 30(5): 12979-12987. DOI: 10.1007/s11356-022-23074-w. [8] Karhunen V, Bakker MK, Ruigrok YM, et al. Modifiable risk factors for intracranial aneurysm and aneurysmal subarachnoid hemorrhage: a Mendelian randomization study[J]. J Am Heart Assoc, 2021, 10(22): e022277. DOI: 10.1161/JAHA.121.022277. [9] Tian DY, Zhang LJ, Zhuang ZH, et al. A two-sample Mendelian randomization analysis of modifiable risk factors and intracranial aneurysms[J]. Sci Rep, 2022, 12(1): 7659. DOI: 10.1038/s41598-022-11720-9. [10] Sun XH, Liu B, Chen Y, et al. Modifiable risk factors for intracranial aneurysms: evidence from genetic studies[J]. Int J Stroke, 2022, 17(10): 1107-1113. DOI: 10.1177/17474930211065640. [11] Zhang ZZ, Wang MM, Yuan S, et al. Genetically predicted coffee and tea consumption and risk of intracranial aneurysm[J]. Eur J Clin Nutr, 2023, 77(8): 811-814. DOI: 10.1038/s41430-023-01295-7. [12] Ma CC, Zhang WW, Mao L, et al. Hyperhomocysteinemia and intracranial aneurysm: a Mendelian randomization study[J]. Front Neurol, 2022, 13: 948989. DOI: 10.3389/fneur.2022.948989. [13] Wen ZH, Feng X, Tong X, et al. A Mendelian randomisation, propensity score matching study to investigate causal association between serum homocysteine and intracranial aneurysm[J]. Stroke Vasc Neurol, 2024, 9(3): 202-211. DOI: 10.1136/svn-2023-002414. [14] Larsson SC, Gill D. Association of serum magnesium levels with risk of intracranial aneurysm: a Mendelian randomization study[J]. Neurology, 2021, 97(4): e341-e344. DOI: 10.1212/WNL.0000000000012244. [15] Yu WJ, Mei YY, Li CF, et al. Predicting the causal relationship between polyunsaturated fatty acids and cerebral aneurysm risk from a Mendelian randomization study[C]//medRxiv, 2023. [16] 刘新志, 吴新龙, 许敏华, 等. 饮酒与颅内动脉瘤关联的孟德尔随机化研究[J]. 心脑血管病防治, 2018, 18(3): 177-180. DOI: 10.3969/j.issn.1009-816x.2018.03.002.Liu XZ, Wu XL, Xu MH, et al. Mendelian randomization study on the association between alcohol drinking and intracranial aneurysms[J]. Prev Treat Cardio Cereb Vasc Dis, 2018, 18(3): 177-180. DOI: 10.3969/j.issn.1009-816x.2018.03.002. [17] Acosta JN, Szejko N, Both CP, et al. Genetically determined smoking behavior and risk of nontraumatic subarachnoid hemorrhage[J]. Stroke, 2021, 52(2): 582-587. DOI: 10.1161/STROKEAHA.120.031622. [18] Zhang ZZ, Yuan S, Larsson SC, et al. Serum calcium, 25-hydroxyvitamin D, and parathyroid hormone levels in relation to aneurysmal subarachnoid hemorrhage[J]. Mol Neurobiol, 2023, 60(6): 3004-3009. DOI: 10.1007/s12035-023-03254-6. [19] Hu LM, Li BY, Liao X, et al. Polymorphisms of inflammatory cytokine genes and risk for intracranial aneurysm: a systematic review and Meta-analysis[J]. Yonsei Med J, 2020, 61(5): 391-399. DOI: 10.3349/ymj.2020.61.5.391. [20] Julian TH, Boddy S, Islam M, et al. A review of Mendelian randomization in amyotrophic lateral sclerosis[J]. Brain, 2022, 145(3): 832-842. DOI: 10.1093/brain/awab420. [21] Skrivankova VW, Richmond RC, Woolf BAR, et al. Strengthening the reporting of observational studies in epidemiology using Mendelian randomization: the STROBE-MR statement[J]. JAMA, 2021, 326(16): 1614-1621. DOI: 10.1001/jama.2021.18236. [22] Spiga F, Gibson M, Dawson S, et al. Tools for assessing quality and risk of bias in Mendelian randomization studies: a systematic review[J]. Int J Epidemiol, 2023, 52(1): 227-249. DOI: 10.1093/ije/dyac149. [23] van de Luitgaarden IAT, van Oort S, Bouman EJ, et al. Alcohol consumption in relation to cardiovascular diseases and mortality: a systematic review of Mendelian randomization studies[J]. Eur J Epidemiol, 2022, 37(7): 655-669. DOI: 10.1007/s10654-021-00799-5. [24] Can A, Castro VM, Ozdemir YH, et al. Association of intracranial aneurysm rupture with smoking duration, intensity, and cessation[J]. Neurology, 2017, 89(13): 1408-1415. DOI: 10.1212/WNL.0000000000004419. [25] Wada H, Ura S, Satoh-Asahara N, et al. α1-Antitrypsin low-density-lipoprotein serves as a marker of smoking-specific oxidative stress[J]. J Atheroscler Thromb, 2012, 19(1): 47-58. DOI: 10.5551/jat.9035. [26] McEvoy JW, Nasir K, DeFilippis AP, et al. Relationship of cigarette smoking with inflammation and subclinical vascular disease: the Multi-Ethnic Study of Atherosclerosis[J]. Arterioscler Thromb Vasc Biol, 2015, 35(4): 1002-1010. DOI: 10.1161/ATVBAHA.114.304960. [27] Yang SZ, Liu QY, Yang JH, et al. Increased levels of serum IL-15 and TNF-β indicate the progression of human intracranial aneurysm[J]. Front Aging Neurosci, 2022, 14: 903619. DOI: 10.3389/fnagi.2022.903619. [28] Vlak MHM, Rinkel GJE, Greebe P, et al. Trigger factors and their attributable risk for rupture of intracranial aneurysms: a case-crossover study[J]. Stroke, 2011, 42(7): 1878-1882. DOI: 10.1161/STROKEAHA.110.606558. [29] Grant RA, Cord BJ, Kuzomunhu L, et al. Aneurysmal subarachnoid hemorrhage and severe, catheter-induced vasospasm associated with excessive consumption of a caffeinated energy drink[J]. Interv Neuroradiol, 2016, 22(6): 674-678. DOI: 10.1177/1591019916660868. [30] Wang Q, Zhang JS, Zhao K, et al. Hyperhomocysteinemia is an independent risk factor for intracranial aneurysms: a case-control study in a Chinese Han population[J]. Neurosurg Rev, 2020, 43(4): 1127-1134. DOI: 10.1007/s10143-019-01138-9. [31] Xi H, Zhang YL, Xu YJ, et al. Caspase-1 inflammasome activation mediates homocysteine-induced pyrop-apoptosis in endothelial cells[J]. Circ Res, 2016, 118(10): 1525-1539. DOI: 10.1161/CIRCRESAHA.116.308501. [32] Can A, Rudy RF, Castro VM, et al. Low serum calcium and magnesium levels and rupture of intracranial aneurysms[J]. Stroke, 2018, 49(7): 1747-1750. DOI: 10.1161/STROKEAHA.118.020963. [33] Reid IR, Bristow SM, Bolland MJ. Cardiovascular complications of calcium supplements[J]. J Cell Biochem, 2015, 116(4): 494-501. DOI: 10.1002/jcb.25028. [34] Zheng SF, Lin P, Lin ZY, et al. Lower serum iron and hemoglobin levels are associated with acute seizures in patients with ruptured cerebral aneurysms[J]. Neurocrit Care, 2019, 31(3): 501-506. DOI: 10.1007/s12028-019-00746-z. -

 点击查看大图
点击查看大图
图(1) / 表(2)
计量
- 文章访问数: 7
- HTML全文浏览量: 5
- PDF下载量: 0
- 被引次数: 0