

The effect of unhealthy lifestyle on the association between adverse childhood experiences and multimorbidity
-
摘要:
目的 探讨童年不良经历(adverse childhood experiences, ACEs)对中老年人共病患病的影响,并进一步分析不健康生活方式在两者关系中的中介效应。 方法 选取2011―2018年中国健康与养老追踪调查队列中的7 513名年龄≥45岁的个体作为研究对象。收集研究对象的年龄和性别等基本资料、ACEs情况、不健康生活方式及慢性非传染性疾病患病资料。采用t检验或χ2检验比较不同特征的中老年人共病患病情况差异,采用非条件logistic回归分析ACEs和不健康生活方式对中老年人共病患病的影响,采用Bootstrap程序检验中介效应。 结果 7 513名研究对象共病患病率为36.34%(95% CI: 35.25%~37.44%)。多因素分析显示,每增加1种ACEs,中老年人共病患病风险增加10.4%(95% CI: 1.058~1.152);与经历1种ACEs的中老年人相比,经历3种和≥4种ACEs的中老年人共病患病风险分别增加38.3%(95% CI: 1.023~1.870)和43.2%(95% CI: 1.065~1.926);每增加1种不健康生活方式,中老年人共病患病风险增加14.4%(95% CI: 1.077~1.216)。与有健康生活方式的中老年人相比,存在≥4种不健康生活方式的中老年人共病患病风险增加99.1%(95% CI: 1.365~2.903)。中介效应分析发现,不健康生活方式的中介效应均无统计学意义(均P>0.05)。 结论 ACEs与中老年人共病患病呈正相关,尚未发现不健康生活方式在中老年人ACEs和共病关联中起中介作用。 Abstract:Objective This study aimed to examine the association between adverse childhood experiences (ACEs) and multimorbidity in middle-aged and older adults, and to investigate whether unhealthy lifestyle mediates this relationship. Methods We analyzed data from 7 513 participants aged ≥45 years in the China Health and Retirement Longitudinal Study from 2011 to 2018. Demographic characteristics, ACEs exposure, unhealthy lifestyle behaviors and chronic disease diagnoses were assessed. Group differences in multimorbidity prevalence were evaluated using t-tests or χ2 tests. Unconditional logistic regression models quantified the effects of ACEs and lifestyle on multimorbidity. Mediation analysis was conducted using the Bootstrap method. Results The prevalence of multimorbidity among the 7 513 participants was 36.34% (95% CI: 35.25%-37.44%). Multivariate analysis revealed that each additional ACE was associated with an 10.4% increase in the risk of multimorbidity (95% CI: 1.058-1.152). Compared to individuals with one ACE, those with 3 and ≥4 ACEs had 38.3% (95% CI: 1.023-1.870) and 43.2% (95% CI: 1.065-1.926) higher risks of multimorbidity, respectively. Additionally, each additional unhealthy lifestyle behavior increased multimorbidity risk by 14.4% (95% CI: 1.077-1.216). Compared to those with healthy lifestyles, individuals with ≥4 unhealthy behaviors had a 99.1% higher risk (95% CI: 1.365-2.903). Mediation analysis revealed that unhealthy lifestyle did not have a significant mediating effect on multimorbidity in middle-aged and older adults (all P>0.05) Conclusions ACEs were positively correlated with multimorbidity, no significant mediating role of an unhealthy lifestyle was found between ACEs and multimorbidity among middle-aged and older adults. -

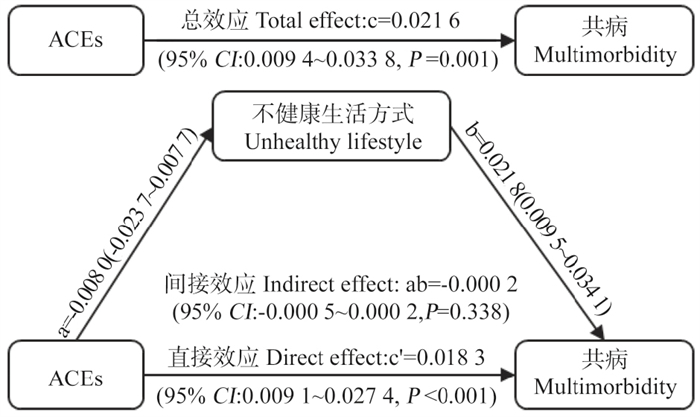
图 1 不健康生活方式在ACEs和共病关联中的中介效应路径图
ACEs: 童年不良经历。
Figure 1. Path diagram of the mediation effect of unhealthy lifestyles in the association between ACEs and multimorbidity
ACEs: adverse childhood experiences.
表 1 研究对象基本特征
Table 1. Basic characteristics of the study participants
变量 Variable 例数
Number of examples共病 Multimorbidity② 患病率
Prevalence/%t/χ2值
valueP值
value否 No 是 Yes 年龄/岁 Age/years① 7 513 63.09±8.97 64.73±8.95 7.635 < 0.001 性别 Gender 1.744 0.187 男 Male 3 590 2 313(48.36) 1 277(46.78) 35.57 女 Female 3 923 2 470(51.64) 1 453(53.22) 37.04 民族 Ethnicity 8.156 0.004 汉 Han 6 996 4 484(93.75) 2 512(92.01) 35.91 少数民族 Ethnic minority 517 299(6.25) 218(7.99) 42.17 婚姻状况 Marital status 3.461 0.063 已婚 Married 5 881 3 776(78.95) 2 105(77.11) 35.79 其他 Other 1 632 1 007(21.05) 625(22.89) 38.30 文化程度 Education 4.951 0.175 小学以下 Primary school 3 333 2 082(43.53) 1 251(45.82) 37.53 小学 Primary school 1 593 1 013(21.18) 580(21.25) 36.41 初中 Middle 1 689 1 111(23.23) 587(21.50) 34.75 高中及以上 Senior high school or up 889 577(12.06) 312(11.43) 35.10 居住地 Residence 1.008 0.315 农村 Rural 4 934 3 161(66.09) 1 773(64.95) 35.93 城市 Urban 2 579 1 622(33.91) 957(35.05) 37.11 职业 Occupation 7.729 0.005 农业 Agricultural 4 767 2 979(62.28) 1 788(65.49) 37.51 非农业 Non-agricultural 2 746 1 804(37.72) 942(34.51) 34.30 自评健康 Self-rated health 308.342 < 0.001 好 Good 2 076 1 649(34.48) 427(15.64) 20.57 差 Poor 5 437 3 134(65.52) 2 303(84.36) 42.36 家庭人均支出水平 The level of expenditure per household 4.643 0.031 低 Low 4 819 3 111(65.04) 1 708(62.56) 35.44 高 High 2 694 1 672(34.96) 1 022(37.44) 37.94 吸烟 Smoking 4.869 0.027 否 No 5 111 3 211(67.13) 1 900(69.60) 37.17 是 Yes 2 402 1 572(32.87) 830(30.40) 34.55 饮酒 Drinking 4.092 0.043 否 No 5 185 3 262(68.20) 1 923(70.44) 37.09 是 Yes 2 328 1 521(31.80) 807(29.56) 34.66 BMI/(kg·m-2) 52.801 < 0.001 < 18.5 464 305(6.38) 159(5.82) 34.27 18.5~<24.0 4 280 2 861(59.81) 1 419(51.98) 33.15 ≥24.0 2 769 1 617(33.81) 1 152(42.20) 41.60 睡眠时间 Sleep time/h 15.399 < 0.001 < 7 2 873 1 750(36.59) 1 123(41.13) 39.09 7~8 1 555 1 023(21.39) 532(19.49) 34.21 >8 3 085 2 010(42.02) 1 075(39.38) 34.84 注:①以x±s表示;②以人数(占比/%)表示。
Note: ① x±s; ② Number of people(proportion/%). 下载: 导出CSV
下载: 导出CSV
表 2 不同童年不良经历的中老年人共病患病情况比较
Table 2. Comparison of multimorbidity prevalence among middle-aged and elderly adults with different adverse childhood experiences
变量 Variable 例数
Number of examples共病 Multimorbidity① 患病率
Prevalence/%χ2值
valueP值
value否 No 是 Yes 感到孤独 Feel alone 11.878 0.001 是 Yes 1 504 900(18.82) 604(22.12) 40.16 否 No 6 009 3 883(81.18) 2 126(77.88) 35.38 欺凌 Bullying 3.745 0.053 是 Yes 1 070 653(13.65) 417(15.27) 38.97 否 No 6 443 4 130(86.35) 2 313(84.73) 35.90 和父母关系 Relationship with parents 0.037 0.848 坏 Poor 1 730 1 098(22.96) 632(23.15) 36.53 好 Good 5 783 3 685(77.04) 2 098(76.85) 36.28 和邻居关系 Relationship with neighbors 7.637 0.006 坏 Poor 1 025 613(12.82) 412(15.09) 40.20 好 Good 6 488 4 170(87.18) 2 318(84.91) 35.73 和朋友关系 Relationship with friends 2.649 0.104 坏 Poor 3 809 2 391(49.99) 1 418(51.94) 37.23 好 Good 3 704 2 392(50.01) 1 312(48.06) 35.42 自我报告健康状况 Self-reported health 5.197 0.023 坏 Poor 771 462(9.66) 309(11.32) 40.08 好 Good 6 742 4 321(90.34) 2 421(88.68) 35.91 健康限制 Health limitation 16.231 < 0.001 是 Yes 541 301(6.29) 240(8.79) 44.36 否 No 6 972 4 482(93.71) 2 490(91.21) 35.71 父母去世 Death of parents 7.036 0.008 是 Yes 1 342 812(16.98) 530(19.41) 39.49 否 No 6 171 3 971(83.02) 2 200(80.59) 35.65 兄弟姐妹去世 Death of siblings 2.064 0.151 是 Yes 1 454 902(18.86) 552(20.22) 37.96 否 No 6 059 3 881(81.14) 2 178(79.78) 35.95 身体虐待 Physical abuse 1.667 0.197 是 Yes 2 143 1 340(28.02) 803(29.41) 37.47 否 No 5 370 3 443(71.98) 1 927(70.59) 35.88 父母精神问题 Parents mental health 17.836 < 0.001 是 Yes 1 470 866(18.11) 604(22.12) 41.09 否 No 6 043 3 917(81.89) 2 126(77.88) 35.18 饥饿 Hunger 39.070 < 0.001 是 Yes 5 660 3 491(72.99) 2 169(79.45) 38.32 否 No 1 853 1 292(27.01) 561(20.55) 30.28 童年社区安全 Childhood neighborhood safety 7.766 0.005 坏 Poor 609 356(7.44) 253(9.27) 41.54 好 Good 6 904 4 427(92.56) 2 477(90.73) 35.88 家庭暴力 Domestic violence 11.919 0.001 是 Yes 486 274(5.73) 212(7.77) 43.62 否 No 7 027 4 509(94.27) 2 518(92.23) 35.83 父母分居或离婚 Parental separation or divorce 1.704 0.192 是 Yes 51 28(0.59) 23(0.84) 45.10 否 No 7 462 4 755(99.41) 2 707(99.16) 36.28 注:①以人数(占比/%)表示。
Note: ① Number of people(proportion/%).
下载: 导出CSV
表 3 ACEs与共病关联的多因素分析
Table 3. Multivariate analysis of the association between ACEs and multimorbidity
ACEs 模型1 Model 1 模型2 Model 2 模型3 Model 3 OR值
value (95% CI)P值
valueOR值
value (95% CI)P值
valueOR值
value (95% CI)P值
valueACEs 1.123(1.078~1.169) < 0.001 1.096(1.050~1.143) 0.001 1.104(1.058~1.152) 0.001 0 1.000 1.000 1.000 1 1.076 (0.797~1.453) 0.634 1.017(0.747~1.384) 0.915 1.015(0.744~1.384) 0.927 2 1.351 (1.010~1.807) 0.042 1.246(0.924~1.679) 0.149 1.256(0.930~1.696) 0.137 3 1.477 (1.104~1.976) 0.009 1.355(1.004~1.828) 0.047 1.383(1.023~1.870) 0.035 ≥4 1.590 (1.197~2.112) 0.001 1.401(1.044~1.880) 0.025 1.432(1.065~1.926) 0.017 注:ACEs,童年不良经历;模型1调整年龄与性别;模型2调整年龄、性别、民族、婚姻状况、文化程度、居住地、职业、自评健康和家庭人均支出水平;模型3在模型2的基础上调整了吸烟、饮酒、BMI和睡眠时间。
Note: ACEs, adverse childhood experiences; Model 1 adjusted for age and gender; Model 2 adjusted for age, gender, ethnicity, marital status, education level, residence, occupation, self-rated health, and per capita household expenditure; Model 3 further adjusted for smoking, drinking, BMI, and sleep status, based on model 2.
下载: 导出CSV
表 4 不健康生活方式与中老年人共病患病的logistic回归分析
Table 4. Logistic regression analysis of unhealthy lifestyles and multimorbidity among middle-aged and elderly adults
不健康生活方式得分
Unhealthy lifestyle score模型1 Model 1 模型2 Model 2 模型3 Model 3 OR值
value (95% CI)P值
valueOR值
value (95% CI)P值
valueOR值
value (95% CI)P值
value得分 Score 1.141(1.075~1.210) < 0.001 1.142(1.075~1.213) < 0.001 1.144(1.077~1.216) < 0.001 0 1.000 1.000 1.000 1 1.204(0.981~1.477) 0.075 1.186(0.963~1.462) 0.108 1.177(0.955~1.451) 0.126 2 1.429(1.167~1.750) 0.001 1.413(1.148~1.737) 0.001 1.407(1.143~1.731) 0.001 3 1.411(1.114~1.787) 0.004 1.395(1.096~1.776) 0.007 1.397(1.097~1.779) 0.007 ≥4 1.972(1.366~2.847) < 0.001 1.993(1.367~2.905) < 0.001 1.991(1.365~2.903) < 0.001 注:模型1调整年龄与性别;模型2调整年龄、性别、民族、婚姻状况、文化程度、居住地、职业、自评健康和家庭人均支出水平;模型3在模型2的基础上调整了ACEs。
Note: Model 1 adjusted for age and gender; Model 2 adjusted for age, gender, ethnicity, marital status, education level, residence, occupation, self-rated health, and per capita household expenditure; Model 3 further adjusted for ACEs, based on model 2.
下载: 导出CSV
表 5 BMI在ACEs和共病关联中的间接效应检验
Table 5. Test of the indirect effect of BMI in the association between ACEs and multimorbidity
效应类型 Effect type 中介效应值 Point estimate Boot标准误Bootstrap sx 95% CI P值 value 总效应 Total effect 0.019 3 0.004 6 (0.010 2~0.028 4) < 0.001 直接效应 Direct effect 0.021 2 0.004 6 (0.012 1~0.030 3) < 0.001 间接效应 Indirect effect -0.001 9 0.000 5 (-0.003 0~-0.000 9) < 0.001 注:ACEs,童年不良经历。
Note: ACEs, adverse childhood experiences.
下载: 导出CSV
-
[1] World Health Organization. The world health report 2008: primary health cared now more than ever[M]. New York: the World Health Report, 2008: 148. [2] Hu YD, Wang ZX, He HJ, et al. Prevalence and patterns of multimorbidity in China during 2002-2022: a systematic review and Meta-analysis[J]. Ageing Res Rev, 2024, 93: 102165. DOI: 10.1016/j.arr.2023.102165. [3] Munyombwe T, Dondo TB, Aktaa S, et al. Association of multimorbidity and changes in health-related quality of life following myocardial infarction: a UK multicentre longitudinal patient-reported outcomes study[J]. BMC Med, 2021, 19(1): 227. DOI: 10.1186/s12916-021-02098-y. [4] Fu Y, Chen MS, Si L. Multimorbidity and catastrophic health expenditure among patients with diabetes in China: a nationwide population-based study[J]. BMJ Glob Health, 2022, 7(2): e007714. DOI: 10.1136/bmjgh-2021-007714. [5] Luo Y, Chen YM, Wang KP, et al. Associations between multimorbidity and frailty transitions among older Americans[J]. J Cachexia Sarcopenia Muscle, 2023, 14(2): 1075-1082. DOI: 10.1002/jcsm.13197. [6] Lin L, Wang HH, Lu CY, et al. Adverse childhood experiences and subsequent chronic diseases among middle-aged or older adults in China and associations with demographic and socioeconomic characteristics[J]. JAMA Netw Open, 2021, 4(10): e2130143. DOI: 10.1001/jamanetworkopen.2021.30143. [7] Al Azri Z, Al-Abri K, Al Sawafi A, et al. Adverse childhood experiences and risky behaviors in Oman: a cross-sectional study[J]. Prev Med Rep, 2024, 5(44): 102809. DOI: 10.1016/j.pmedr.2024.102809. [8] Xu HQ, Zhang XY, Wang JJ, et al. Exploring associations of adverse childhood experiences with patterns of 11 health risk behaviors in Chinese adolescents: focus on gender differences[J]. Child Adolesc Psychiatry Ment Health, 2023, 17(1): 26. DOI: 10.1186/s13034-023-00575-1. [9] Brugiavini, A., Buia RE., Kovacic M, et al. Adverse childhood experiences and unhealthy lifestyles later in life: evidence from SHARE countries[J]. Rev Econ Househ, 2023, 21(1): 1-18. DOI: 10.1007/s11150-022-09612-y. [10] 中华人民共和国国家卫生和计划生育委员会. 成人体重判定: WS/T 428-2013[S]. 北京: 中国标准出版社, 2013: 1-2.National Health and Family Planning Commission of the PRC. Adult weight assessment: WS/T 428-2013[S]. Beijing: Standards Press of China, 2013: 1-2. [11] 中国营养学会. 中国居民膳食指南(2022)[M]. 北京: 人民卫生出版社, 2022: 94-95.Chinese Nutrition Society. Dietary guidelines for Chinese residents(2022)[M]. Beijing: People's Medical Publishing House, 2022: 94-95. [12] Svensson T, Saito E, Svensson AK, et al. Association of sleep duration with all-and major-cause mortality among adults in Japan, China, Singapore, and Korea[J]. JAMA Netw Open, 2021, 4(9): e2122837. DOI: 10.1001/jamanetworkopen.2021.22837. [13] 温忠麟, 叶宝娟. 中介效应分析: 方法和模型发展[J]. 心理科学进展, 2014, 22(5): 731-745.Wen ZL, Ye BJ. Mediation effect analysis: methods and model development[J]. Adv Psychol Sci, 2014, 22(5): 731-745. [14] Ornish D, Madison C, Kivipelto M, et al. Effects of intensive lifestyle changes on the progression of mild cognitive impairment or early dementia due to Alzheimer's disease: a randomized, controlled clinical trial[J]. Alzheimers Res Ther, 2024, 16(1): 122. DOI: 10.1186/s13195-024-01482-z. [15] Han YT, Hu YZ, Yu CQ, et al. Lifestyle, cardiometabolic disease, and multimorbidity in a prospective Chinese study[J]. Eur Heart J, 2021, 42(34): 3374-3384. DOI: 10.1093/eurheartj/ehab413. [16] Sanaya N, Janusaite M, Dalamaga M, et al. The physiological effects of weight-cycling: a review of current evidence[J]. Curr Obes Rep, 2024, 13(1): 35-50. DOI: 10.1007/s13679-023-00539-8. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 1
- HTML全文浏览量: 2
- PDF下载量: 0
- 被引次数: 0